
An ED screening and diagnostic testing program found a high prevalence of hepatitis C. Results suggest that continued efforts are needed to develop and evaluate policies for ED-based hepatitis C screening.
Hepatitis C virus affects about 3 million Americans and is a leading cause of end-stage liver disease, hepatocellular carcinoma, and liver transplants. National recommendations endorse using risk-based hepatitis C screening, which includes screening patients with a history of injection drug use as well as one-time screenings of “baby boomers,” or patients born between 1945 and 1965. Current data suggest that the baby boomer generation accounts for 75% of people infected with hepatitis C, but 1.25 to 1.75 million of them are unaware that they are infected.
“Hepatitis C screening has long been considered impractical for EDs, but advances in rapid testing technology, the development of new therapies, and improvements in reimbursement for selective screening has created new opportunities to implement these screenings in the ED setting,” says Douglas A.E. White, MD. Despite these advances, clinical experience with hepatitis C virus screening in EDs is limited.
Testing a New Program
Recently, Dr. White and colleagues at Alameda Health System implemented an ED-based screening program for both HIV and hepatitis C into the triage process according to recommendations from the CDC and United States Preventive Services Task Force. As an adjunct to screening, physicians could order HIV and hepatitis C testing when clinically indicated. For a study published in Annals of Emergency Medicine, the research team reported results of the hepatitis C portion of this screening program. The primary objective was to determine the prevalence of hepatitis C among tested patients, but the authors also evaluated factors associated with testing positive.
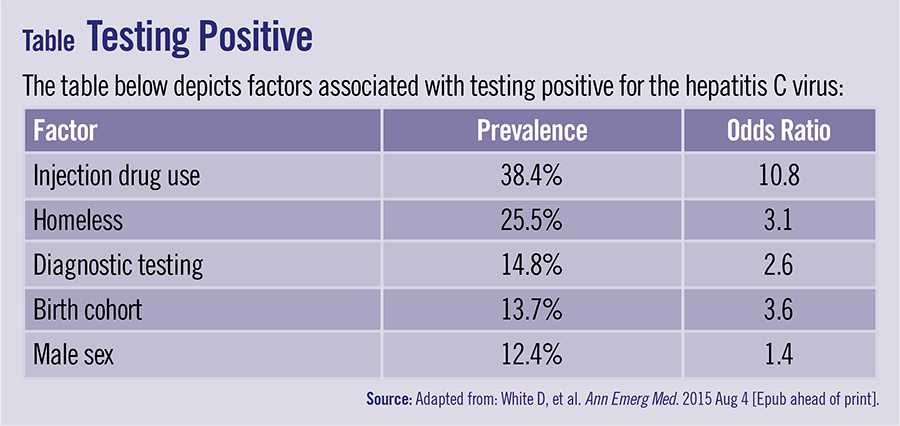
Of the more than 26,000 unique adults who presented to the ED during the study period, almost 10% completed hepatitis C screening or diagnostic testing. “Among these individuals, 10% were antibody positive,” says Dr. White. Several factors were associated with testing positive for hepatitis C, including using injection drugs, being homeless, and receiving diagnostic testing, among others (Table). For those testing positive for the hepatitis C antibody, more than half had documentation of their results being disclosed and two-thirds had confirmatory ribonucleic acid testing performed, of whom 70% had a positive result. Follow-up appointments at the hepatitis C virus clinic were arranged for 45% patients with confirmed positive results.
“During our integrated ED screening program, the prevalence of testing positive for hepatitis C was high across all patient groups that were screened, including those outside of the CDC-recommended risk cohorts,” Dr. White says. “Although we screened fewer patients than expected, the results highlight the importance of the ED as a venue for hepatitis C virus testing.”
Overcoming Challenges
Despite demonstrating high rates of hepatitis C antibody reactivity among nearly all subgroups tested, the study noted that triage nurses often deviated from the protocol, frequently failed to assess injection drug use risk, and regularly offered screening to patients who were not baby boomers. The discrepancy between the number of accepted screening tests and number of tests actually performed is not unusual, and a variety of factors may be at play. For example, not all patients had blood drawn and some were discharged before venipuncture could take place. Informal discussions with nurses also revealed they often forgot to order the hepatitis C test, citing that they didn’t feel familiar with test ordering or found the process to be inconvenient.
The study also revealed that many patients testing positive for hepatitis C were discharged before having their results disclosed and before confirmatory tests could be conducted. This finding illustrates the importance of increasing the availability of positive test results before discharge and improving laboratory-to-physician communication. These efforts are needed for faster test processing and to improve discharge follow-up protocols.
Dr. White and colleagues also noted that it was difficult to link newly-diagnosed patients to care for hepatitis C. “It takes time to contact patients and arrange follow-up,” he says. “Even with efforts to streamline processes, appointment non-attendance rates were still high, meaning that ongoing outreach and surveillance is required.” The study notes that, in addition, not all patients with reactive hepatitis C tests required immediate referral to a specialist. Referral mechanisms will be site specific and depend on access to care and other resources.
A Worthwhile Effort
Reimbursement for hepatitis C screening presents a significant challenge, according to Dr. White. “Despite this challenge, our findings highlight the significant burden of hepatitis C among patients receiving ED care. EDs can play a critical role in identifying patients with undiagnosed disease, and these are worthwhile efforts considering the growing burden of hepatitis C in the U.S. More resources are needed to support efforts to develop and evaluate policies for ED-based hepatitis C screening and diagnostic testing.” The study group noted that future studies should focus efforts on examining risk- and non-risk-based approaches to hepatitis C screening.
 PWeekly
PWeekly
{kind=link}