

In order for the economic stability of the United States healthcare system to improve, hospitals throughout the country are striving to deliver high-quality care while containing cost. Current estimates suggest that the proportion of adults aged 65 and older will exceed 20% by 2030. This creates a need for the development of strategies that improve patient-centered care for older patients while reducing costs. Another important consideration in this patient population is reducing adverse outcomes resulting from hospitalization.
In an effort to address care for older patients, many hospitals throughout the U.S. have been developing Acute Care for Elders (ACE) units for the past 20 years. These units use an interdisciplinary team model to provide hospital care as opposed to a multidisciplinary model. “An interdisciplinary model integrates disciplines to collaboratively develop patient-centered care plans,” explains Kellie L. Flood, MD. “With multidisciplinary models, providers from all disciplines deliver care, but tend to practice independently or operate in silos.”
The primary purpose of the ACE model is to reduce adverse outcomes in older adults with frequent interdisciplinary team rounds. During these rounds, geriatric syndromes are recognized and managed, while transition planning is initiated from the day of admission. In previous studies, ACE units have been shown to improve processes of care, prescribing practices, physical functioning, and patient and provider satisfaction. These analyses have also suggested that ACE units help reduce rates of restraint use and institutionalization.

Assessing the ACE Model
To gain better perspective on the value of ACE models, Dr. Flood and colleagues at the University of Alabama at Birmingham published a study in JAMA Internal Medicine that examined variable direct costs from an interdisciplinary ACE unit and compared it with a multidisciplinary usual care (UC) unit. For the study, the investigators assessed hospitalists’ patients aged 70 and older who spent their entire hospitalization in either the ACE or UC unit. Using administrative data, variable direct costs for ACE and UC patients were analyzed. The study group also conducted a subset analysis that was restricted to the 25 most common diagnosis-related groups (DRGs) shared by ACE and UC patients.
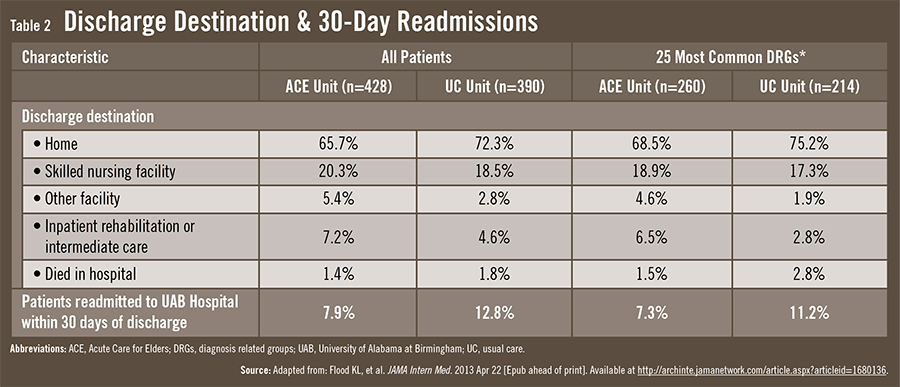
The ACE unit team model was shown to reduce costs and 30-day readmissions. For all DRGs, the average variable direct cost per patient was $2,109 for ACE, compared with $2,480 for UC (Table 1). On average, the ACE unit saw a variable direct cost savings of $371 per patient over the UC patient group, a potential savings of $148,000 for every 400 patients. Furthermore, fewer ACE patients were readmitted within 30 days of discharge (Table 2). The study team noted that the university incurred no additional costs for care process development, and that their ACE unit had not undergone any environmental modifications.
“The ACE unit concept provides evidence-based geriatric care at reduced cost.”
“These data is important because few analyses have evaluated cost as the primary outcome of an ACE unit as compared with a UC unit that uses the same attending physicians and unit staffing,” adds Dr. Flood. “The study patients were evenly matched in terms of age, gender, comorbidities, length of stay, and staff-to-patient ratio. Our head-to-head comparison showed that the ACE unit concept provides evidence-based geriatric care at reduced cost.”
Significant Implications
A key component of the ACE unit concept is the daily team meeting, which links geriatricians and nurse coordinators to each patient’s own nurse and care team. Healthcare professionals from every field that may have a role in treatment are represented, including physical and occupational therapists, dietitians, pharmacists, social workers, chaplains, and volunteers. “Geriatric patients admitted for acute illnesses often have comorbid conditions and may be taking multiple medications,” says Dr. Flood. “The daily team meetings and ACE unit concepts help to increase the recognition of factors that can adversely impact their hospitalization and foster more appropriate care.”
Dr. Flood notes that much attention in U.S. healthcare is being paid to improving care processes while reducing costs and 30-day readmissions. “This is a vital objective for the Medicare program and our nation as a whole,” she says. “The ACE model meets these goals. Results from previous research show that ACE units improve the functional abilities of hospitalized geriatric patients and simultaneously reduce length of stay and long-term care placement.”
In light of the findings, Dr. Flood says the next step is to better disseminate the ACE unit concept to hospitals across the country. “The ACE unit concept takes buy-in from all constituents. They should recognize that this is a win-win scenario. It’s a win for the healthcare system by reducing costs and lowering readmission rates, and it’s a win for patients because they’re receiving better care.”
 admin
admin
{kind=link}
{kind=link}