

Studies have shown that distress is common among people with cancer, but the types and causes vary. “Research shows that 20% to 25% of newly diagnosed cancer patients and/or survivors are at risk for mood or anxiety disorders, but these problems can go undetected unless they’re considered to be a possibility and then evaluated,” says Barbara L. Andersen, PhD. The days surrounding the diagnosis and initiation of cancer treatment tend to be the most stressful for patients. Failing to address psychological needs, regardless of when they arise, can increase risks for stress and anxiety as well as depressive symptoms. It can also reduce quality of life, increase risks for adverse effects, and lead to more physical symptoms.
Treatment for anxiety or depression is often successful and has the potential to reduce the risk of cancer recurrence or disease-related death. “Clinicians may not be able to prevent some of the chronic or late medical effects of cancer, but we can play a vital role in preventing or reducing the emotional fall-out at diagnosis and thereafter,” Dr. Andersen says. If symptoms of anxiety or depression can be recognized and treated effectively, there is a chance that clinicians can reduce the human cost of cancer.
New Recommendations
Recently, the American Society of Clinical Oncology (ASCO) released new guidelines to help manage anxiety and depressive symptoms in adults with cancer. The document is a clinical practice guideline adaptation that incorporates recommendations that have been set forth from other organizations. The guidelines detail optimal strategies for screening and assessing patients and offer options for psychological and supportive care interventions for those experiencing symptoms of depression and/or anxiety.
Vigilance for Screenings & Assessments
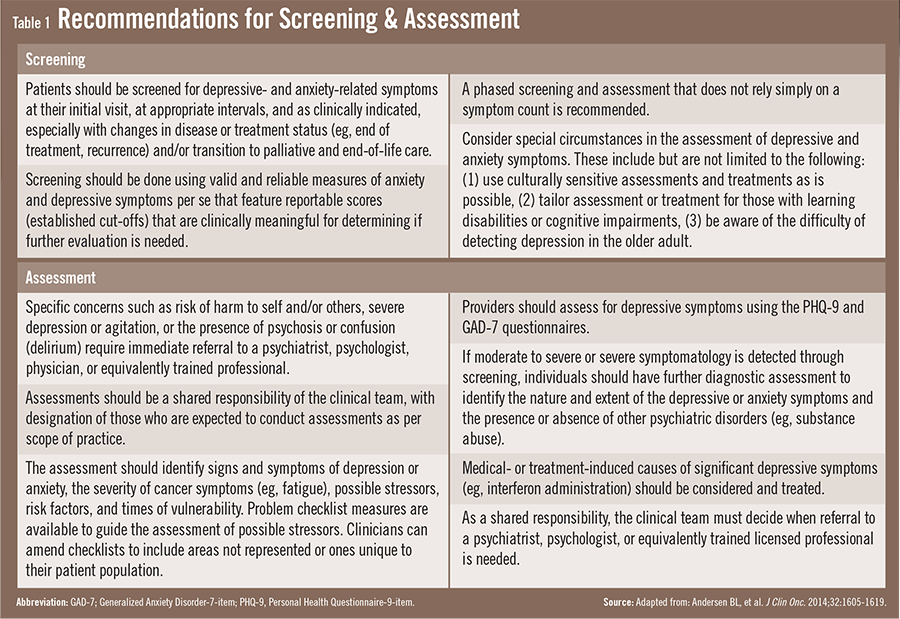
According to the ASCO guidelines, all patients with cancer should be evaluated for symptoms of depression and anxiety periodically across the trajectory of care (Table 1). Assessment should be performed using validated, published measures, and procedures. “Depending on levels of symptoms that are reported, different treatment pathways are suggested,” says Dr. Andersen. “A strong doctor–patient rapport can help when assessing patients’ depression and anxiety and determine the most appropriate treatment strategy. We must also regularly reassess patients’ mental health status to determine the efficacy of the first course of treatment for anxiety or depression. If treatments are ineffective, steps can then be taken in a timely fashion to find alternative treatments or modifications.”
The ASCO guidelines note that healthcare providers should first identify the available resources in their institution and community for treating depression and anxiety symptoms. The availability and accessibility of supportive care services for all patients with cancer are important in efforts to prevent or reduce the severity of symptoms. “Healthcare providers are busy and may not appreciate the impact of depression or anxiety disorders,” Dr. Andersen says. Research shows that psychiatric disorders are more prevalent among patients with cancer than for those with other chronic illnesses. The guidelines emphasize greater vigilance in considering and evaluating depression and anxiety symptoms in patients with cancer.
Continued Follow-Up
For many survivors, the experience of cancer does not end with the conclusion of therapy. Survivors oftentimes have lingering issues that can affect all aspects of their lives, including physical, psychological, social, existential, and financial worries. “This can culminate in added psychological distress,” says Dr. Andersen. In addition, cancer survivors can also experience other chronic comorbid conditions, such as heart disease, diabetes, or age-related problems, like arthritis or osteoporosis. These comorbidities can further impact patients’ emotional well-being and should be addressed in follow-up care.
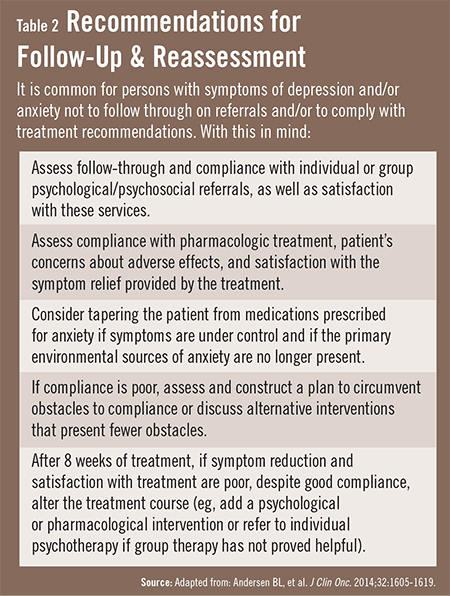
When patients complete cancer therapy, many are transitioned to a primary care physician or other providers for follow-up. This transition, however, may be difficult for some patients. Moreover, survivors with depression or anxiety may not follow through on referrals or comply with treatment recommendations (Table 2). To overcome this hurdle, clinicians are recommended to provide patients with a survivorship care plan that is personalized. “These plans should offer information about treatment and follow-up for patients as well as any new providers,” Dr. Andersen says. “For patients, these plans should identify providers who will be responsible for specific aspects of their physical and emotional healthcare needs in the near future.”
Dr. Andersen notes that cancer survivors are still vulnerable to distress later in life. “We have to remember that these patients can feel the effects emotionally, interpersonally, and financially over time,” she says. “Clinicians must be vigilant about addressing depressive and anxiety symptoms throughout the course of care. The guidelines from ASCO can help us recognize and hopefully eliminate gaps in care for these patients.”
 JonN
JonN
{kind=link}
{kind=link}