

Over the last decade, significant advances and innovations have rapidly evolved in the use of PCI for patients with coronary artery disease (CAD). The American College of Cardiology (ACC)/American Heart Association (AHA), together with the Society for Cardiovascular Angiography and Interventions (SCAI), released a revised clinical guideline for the management of CAD patients undergoing PCI. Published in the December 6, 2011 Journal of the American College of Cardiology, the update emphasizes careful selection of CAD treatment and includes the most extensive section to date on revascularization.
The Heart Team Concept for PCI and CABG
“The heart team includes an interventional cardiologist and a cardiac surgeon who review patient history and anatomy, discuss whether PCI and/or CABG are appropriate, and explain these options in detail with patients before a treatment option is chosen,” says Glenn N. Levine, MD, who chaired the ACC/AHA/SCAI guideline writing committee. The guidelines include a Class I recommendation for utilizing a heart team approach in patients with unprotected left main CAD and/or complex CAD in cases where the optimal revascularization strategy is not straightforward.
New Section on CAD Revascularization
For the first time ever, the CAD revascularization section was developed through a collaboration that involved experts from the ACC, AHA, and SCAI on both PCI and CABG. According to the guidelines, CABG is recommended for improving survival in patients with significant left main coronary artery stenosis, as well as those with significant stenoses in three major coronary arteries or in the proximal left anterior descending artery and one other major coronary artery. CABG or PCI is recommended for survivors of sudden cardiac death with presumed ischemia-mediated ventricular tachycardia caused by significant stenosis in a major coronary artery.
Dr. Levine says “CABG or PCI can improve symptoms in patients with one or more significant coronary artery stenoses that are amenable to revascularization and in whom angina persists despite guideline-adherent care.”
Preprocedural Considerations Before Pursuing PCI
Contrast-induced acute kidney injury (AKI) is one of the most common causes of hospital-acquired AKI, according to Dr. Levine. “Clinicians should be aware of this risk in patients undergoing PCI and proper preprocedural precautions should be taken [Table 1]. Saline hydration and minimizing contrast media are the only methods shown to clearly reduce risk of contrast-induced AKI.”
Some data show that patients with a history of anaphylactoid reaction have a recurrence rate of 16% to 44%. Research, however, has shown that adequate pretreatment can reduce recurrence rates dramatically. When administered within 7 days of PCI, statins seem to reduce the risk of periprocedural myocardial infarction in patients with CAD and acute coronary syndrome (ACS). Because periprocedural bleeding is widely recognized as a major risk factor for subsequent mortality, measures to minimize bleeding complication risks are recommended in the ACC/AHA/SCAI guidelines. “We now have data showing that PCI can be performed successfully at hospitals without on-site cardiac surgical backup when properly planned using strict criteria for the performance of PCI in such situations,” adds Dr. Levine.
Special Populations: Patients with ACS
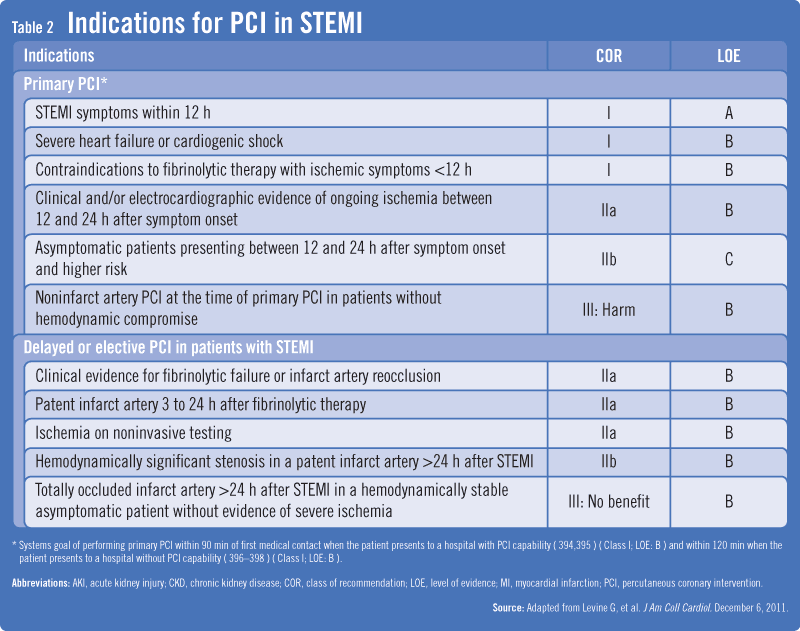
Among patients with unstable angina/NSTEMI, an early invasive strategy is indicated for those with refractory hemodynamic or electrical instability or for those at high risk for clinical events. “The choice between PCI or CABG in patients with ACS should be based on the same considerations as those without ACS,” Dr. Levine says. In patients with STEMI, immediate coronary angiography with intent to perform PCI is recommended for those who are candidates for primary PCI or have severe heart failure or cardiogenic shock and are suitable for revascularization. The guidelines recommend primary PCI for patients within 12 hours of onset who:
Present to a hospital with PCI capability or can be rapidly transported to a hospital that performs PCI.
Develop severe heart failure or cardiogenic shock.
Have STEMI and contraindications to fibrinolytic therapy with ischemic symptoms for less than 12 hours.
For patients with cardiogenic shock, PCI is recommended (Table 2). A hemodynamic support device is recommended after STEMI for those who do not quickly stabilize with pharmacologic therapy.
Stay Tuned for Future PCI Guidelines
“We still have insufficient data to form recommendations for many other aspects of care for these patients, including intracoronary stem cell infusions, designer drugs, optical coherence tomography, virtual histology, and drug-eluting balloons,” says Dr. Levine. “Future PCI guidelines will need to address these and other emerging technologies and treatments.”
 Janine Anthes
Janine Anthes
![[Table 1]](https://www.physiciansweekly.com/wp-content/uploads/2012/07/Levine-Table-1.png){kind=link}
{kind=link}