

Studies show that attrition from general surgery programs is high, even with the introduction of work-hour limitations and new restrictions on hours for general surgery residents. Research has also shown that many factors play a role in residency attrition, most notably lifestyle considerations. Several studies have linked female sex to an increased risk of attrition, but not all research has corroborated this relationship. “Women still represent the minority among surgical residents throughout the United States,” says Erin G. Brown, MD. “There are many stereotypes regarding attrition among female residents, including pregnancy during residency being a risk factor for attrition.”
Exploring the Issue
A significant number of residents report being perceived negatively if they become pregnant during training, according to some investigations. “Since more women are entering medicine, it’s important to examine the potential links between sex, pregnancy, and attrition,” says Dr. Brown. To address this research gap, Dr. Brown and colleagues conducted a study to determine whether child rearing during training increased the risk of attrition from general surgery residency. The study, published in JAMA Surgery, was a retrospective review of general surgery residents at the University of California, Davis over a 10-year period. The study team analyzed voluntary and involuntary attrition rates as well as the incidence of child rearing among residents.
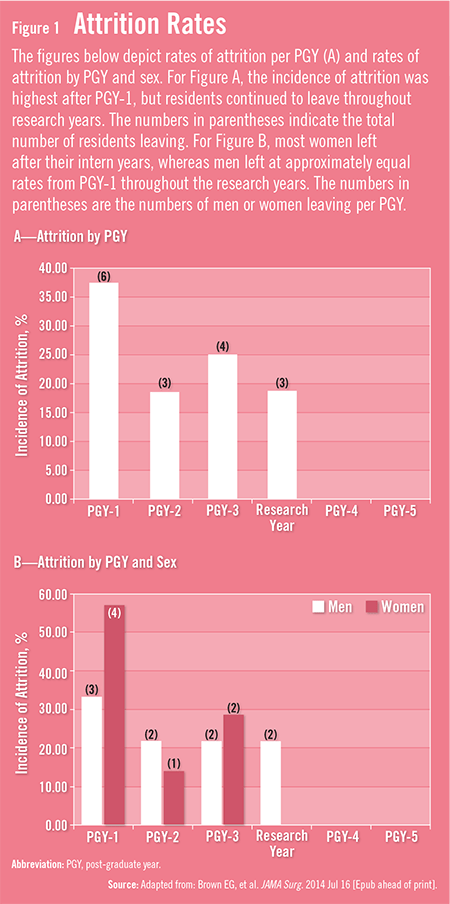
“Our study found that neither sex nor child rearing was a risk factor for attrition in general surgery residencies,” Dr. Brown says. Overall, the attrition rate for women was not significantly different from the proportion of men who left the general surgery residency program. The attrition rate, which was 18.8%, was comparable with rates published in other studies. A higher percentage of women left after their intern year when compared with men (Figure 1). Men also had the highest rate of attrition during research, whereas no women left during research years.
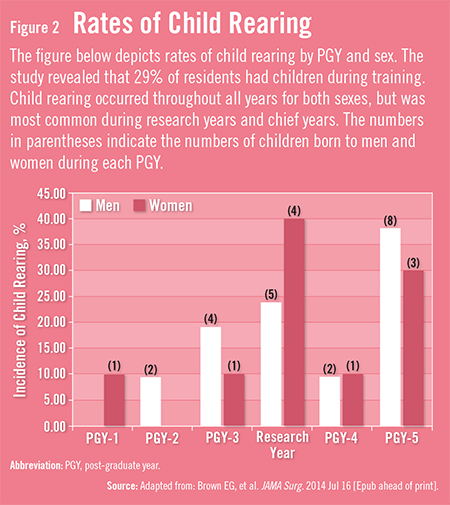
Of the 85 residents assessed in the study, nine women reported a total of 10 pregnancies, and 16 men reported raising 21 children. Women and men choosing to participate in child rearing during training were not at higher risk of attrition. Both men and women were most likely to have children born during research years and their final year of training (Figure 2). “Importantly,” adds Dr. Brown, “residents with children born during their training did not have fewer total case numbers or lower board pass rates when compared with residents who did not have children during their training.” She notes that women who had children during training were more likely to pursue fellowship than those who did not.
A Changing Culture
With more women entering the field of surgery than ever before, Dr. Brown says that any attrition relating to sex differences or child rearing should be carefully examined. “The culture of surgery is changing because there is greater appreciation of the need for a positive work-life balance,” she says. “This includes having a life outside of work and starting a family.” The acceptance of pregnancy during residency is important considering that women are increasingly entering surgical residency during prime childbearing years. The rates of child rearing for both male and female residents have reportedly been rising throughout the U.S.
According to Dr. Brown, adjustments should be made to accommodate maternity and paternity leave even though these life events can place a strain on residency programs. “Institutions should establish written policies for leave and encourage open communication and advanced notice about pregnancy in order to reduce the burden it can place on a residency program,” she says. Such policies may reduce the perceived negative attitudes toward child rearing during training among surgery residents and faculty.
The Family and Medical Leave Act mandates that any woman be granted up to 12 weeks of leave after childbirth, and Dr. Brown says residency programs should create ways to accommodate this maternity leave. “Institutions should prioritize the maintenance of education for residents and strive to avoid overburdening other residents who cover for those taking leave,” she says. She adds that schedule adjustments can be made based on the need for in-house coverage, service volume, number of residents on service, and the length of leave. Residents can also be redistributed to different services when needed. “Efforts should be made to allow residents to take their leave for child rearing without putting undue stress on their peers,” says Dr. Brown. “With the proper institutional support, child rearing during training can be accommodated without putting residents at an increased risk for attrition.”
 TimH
TimH
{kind=link}
{kind=link}