

According to recommendations from the American Diabetes Association, all individuals with diabetes should receive diabetes self-management education and support (DSME/S) when they are diagnosed with the disease and as needed thereafter. Recently, the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics released a joint position statement on DSME/S. Published in Diabetes Care and available at http://care.diabetesjournals.org, the document aims to enhance patients’ experiences with diabetes care and education, improve overall health, and reduce diabetes-associated healthcare costs.
“Currently, there is no consistency with regard to when and how patients with diabetes are referred to DSME/S by their healthcare providers,” says Maggie Powers, PhD, RD, CDE, who was lead author of the joint position statement. “Healthcare providers may also not fully recognize the benefits of DSME/S or how it should be utilized. The joint position statement addresses both of these considerations.”
Research shows that DSME/S can improve A1C levels and have a positive effect on other clinical, psychosocial, and behavioral aspects of diabetes, says Jo Ellen Condon, RD, CDE. “Ultimately, DSME/S helps inform, empower, and engage patients to manage the disease on their own and with their healthcare providers,” she says. “Studies show that DSME/S can help lower A1C levels with just one patient visit to these services. Diabetes is a disease that requires patients to be proficient in many self-management skills, and DSME/S is critical to laying the foundation for long-term management. It helps patients become effective self-managers and assists them with important daily decisions about food, exercise, and medications.”
A Helpful Blueprint
The joint position statement arms healthcare teams with the information required to better understand the educational process and expectations for DSME/S and their integration into routine care. It is recommended that healthcare providers develop processes to guarantee that all patients with type 2 diabetes receive DSME/S services and ensure that adequate resources are available in the community to support these services.
“The joint position statement also provides clinicians with information on reimbursement, national standards for DSME/S, and referring patients to these services,” says Powers. “DSME/S is a covered benefit by Medicare but less than 5% of beneficiaries are actually receiving this service. For those with private insurance, the usage rate is only about 7% in the first year after diagnosis. These figures are disappointing because these services can improve patient outcomes, quality of life, and quality of care measures.”
Key Principles
The joint position statement notes that there are four critical times to assess, provide, and adjust DSME/S:
- With a new diagnosis of type 2 diabetes.
- Annually for health maintenance and preventing complications.
- When new complicating factors influence self-management.
- When transitions in care occur.
The framework for identifying topics to discuss at each time include healthy eating, being active, monitoring, taking medication, problem solving, reducing risks, and healthy coping. This framework can help guide the educational assessment and plan. “It’s important to recognize, however, that situations that require additional attention to self-management needs can arise at any time,” says Powers.
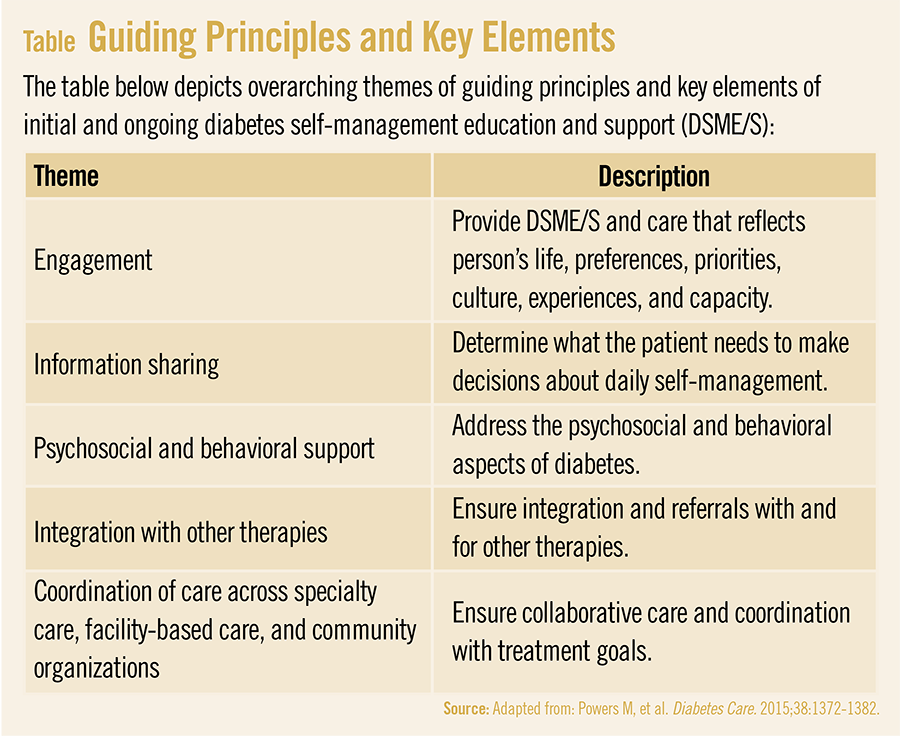
An important component to the joint position statement is its diabetes education algorithm, according to Condon. It provides an evidence-based visual depiction of when to identify and refer individuals with type 2 diabetes to DSME/S. The algorithm relies on five guiding principles and represents how DSME/S should be provided through patient engagement, information sharing, psychosocial and behavioral support, integration with other therapies, and coordinated care (Table).
The position statement notes that taking a patient-centered approach—one in which collaboration and effective communication are the routes to patient engagement—is paramount. This strategy includes eliciting emotions, perceptions, and knowledge through active and reflective listening; asking open-ended questions; exploring the desire to learn or change; and supporting self-efficacy. “Clinicians should view DSME/S as an interactive, personalized approach to care,” says Condon.
Overcoming Barriers
Despite the proven value and effectiveness of DSME/S, a looming threat to the success of these programs is low utilization. “Clinicians need greater awareness of the value of these services, and healthcare providers need to be more willing to refer their patients to them,” says Powers. To increase receipt of DSME/S, it is necessary to consider any and all possible barriers to providing these services. Several barriers are associated with DSME/S adoption, including a misunderstanding of its necessity and effectiveness, confusion on when and how to make referrals, and lack of access to these services. Provider misconceptions on reimbursement or other issues can also limit utilization of DSME/S.
“Patient education and empowerment can be time-consuming for physicians, but DSME/S can serve as an effective support to clinical staff,” says Condon. “Educators can communicate the importance of self-management to achieve treatment and quality-of-life goals and reduce the likelihood of feelings of being overwhelmed.” Processes that support referrals and reimbursement practices are necessary.
Powers notes that the American Diabetes Association and American Association of Diabetes Educators have developed tools to search for DSME/S programs by zip code. She says clinicians should use these tools when referring their patients for these services. Additionally, if a registered dietitian is not available through the DSME/S program, the Academy of Nutrition and Dietetics has resources arranged by zip code for finding a registered dietitian for nutrition therapy.


{kind=link}