

The burden of diagnosed and undiagnosed depression in the United States is significant and well documented, but it can be even more severe for people living with diabetes. Research has shown that the chances of becoming depressed increase as diabetes complications worsen. “Depression can lead to poorer physical and mental functioning and has also been associated with higher mortality in patients with diabetes,” explains William H. Polonsky, PhD, CDE. “Depression can impair the ability to carry out diabetes care tasks and may compromise adherence to diet, exercise, and medication plans.”
The causes that underlie the association between depression and diabetes are also unclear. Data suggest that women, those living with other comorbid conditions (eg, heart disease), and those from poor socioeconomic classes who have diabetes are more likely than others with the disease to suffer from depression. Studies have also shown that diabetics with a history of depression are more likely to develop diabetes-related complications than those without depression.
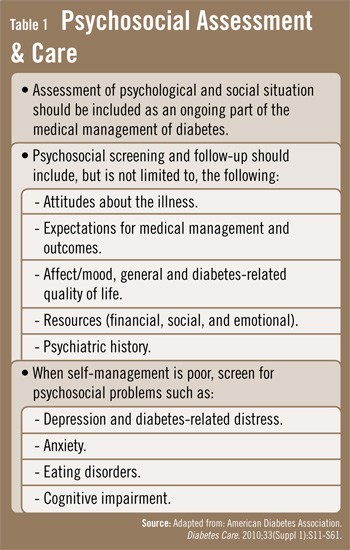
“The key is to recognize that there are opportunities for clinicians to seek out depression in a timely, efficient manner so that these individuals can be identified and, if needed, referred on to appropriate mental health services,” Dr. Polonsky says (Table 1). “Physicians should use the patient-provider relationship as a foundation to increase the likelihood that patients will accept referrals for other services. It’s also important to establish that emotional well-being is a critical part of diabetes management.”
Identifying Depression Early
The American Diabetes Association recommends that physicians incorporate psychological assessments and treatment into routine care rather than wait for the identification of specific problems or deterioration in psychological status. “Several self-administered depression assessment questionnaires are readily available for free, such as the Patient Health Questionnaire-9,” says Dr. Polonsky. “These tools should be incorporated early in the management of patients with diabetes.” Physicians should seize opportunities to screen diabetic patients for their depression status at diagnosis, during regularly scheduled management visits, and during hospitalizations. They should also screen for depression when discovering diabetes-related complications or when problems with glucose control, quality of life, or adherence are identified.
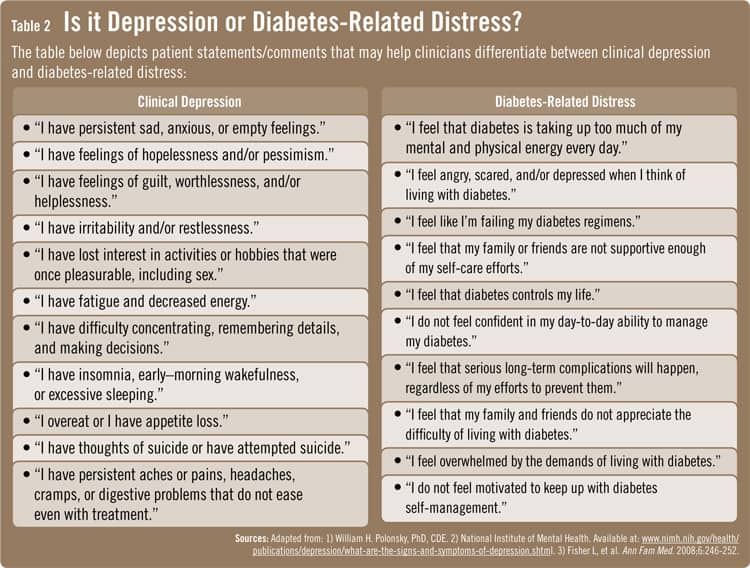
In some cases, patients may experience diabetes-related emotional distress rather than clinical depression, says Dr. Polonsky (Table 2). “It’s important to discern which condition patients have because it will affect how patients should be managed. Researchers have developed brief questionnaires that can help physicians determine if patients are suffering from diabetes-related distress, similar to the scales that have been created for clinical depression. Patients may be vulnerable to diabetes-related distress at any time, especially if they become overwhelmed by diabetes and/or frustrated that the disease cannot be controlled. Other warning signs to consider include when the need for intensified treatment is evident, when complications are discovered, or when medical status worsens. Antidepressants, for example, may be beneficial for those with clinical depression, but they may be less helpful for patients with diabetes-related distress.”
Guiding Patients To Treatment
Treatment for depression may also help people to more easily follow self-care recommendations. In turn, this can have a strong impact on improving quality of life. Treating depression with psychotherapy, medication, or a combination of these treatments may improve patients’ well-being and their ability to manage diabetes and its complications.
“Studies indicate that psychotherapy and antidepressant medications can alleviate depression for the majority of patients with diabetes,” says Dr. Polonsky. “These treatment strategies can have a profound impact on patients’ lives. However, it should be noted that patients must be monitored closely—especially when antidepressants are prescribed. Research suggests that only about half of depressed patients who receive antidepressants will achieve an adequate treatment response. Close monitoring allows physicians to make treatment changes and adjustments when necessary for depression as well as for diabetes so that outcomes can be optimized.”
When treating depression in the context of diabetes, patients may also benefit by receiving care from mental health professionals who are in close communication with physicians who are providing diabetes care. “There are mental health professionals that specialize in treating people with depression and co-occurring physical illnesses,” says Dr. Polonsky. “These specialists should be incorporated in patient care when needed, particularly for patients with diabetes who are at higher risk for depression.” Patients should also be asked to report any herbal supplements that they may be using to address depression. This is critical to ensuring that no harmful interactions occur with other medications involved in diabetes regimens.
Regardless of how the combination of depression and diabetes manifests, finding a path to successful treatment and optimizing access to care are serious issues for these patients. “Costs, insurance access, and restrictions can make treatment difficult or impossible for some people,” Dr. Polonsky says. “However, as more clinical trials are conducted, there is hope that physicians will better appreciate the links between depression and diabetes so that we can more effectively serve these patients and, ultimately, maximize outcomes for both conditions.”
 JonN
JonN
{kind=link}
{kind=link}