

Migraine is one of the most common disorders for which patients seek medical treatment in the ED. Studies show that migraine causes most of the 5 million headache visits to EDs in the United States each year. “The average annual costs for migraine-related ED visits are at least $700 million,” says Mia T. Minen, MD, MPH. “Considering the high costs of ED care of migraines and the fact that the ED environment is typically not conducive to treating these headaches, it’s important for healthcare systems to make efforts to prevent or divert ED migraine visits and take steps to ensure fewer return visits.”
Research suggests that the current state of migraine management in EDs is suboptimal. In the journal Headache, Dr. Minen and colleagues reviewed how patients with migraine are managed in the ED. The analysis identified characteristics of patients seeking ED care for migraine and examined guidelines and current practices regarding ED imaging use for migraine. It also explored how current ED care for migraine deviates from recommended treatment practices and investigated potential methods for improving outcomes following ED treatment.
Characterizing Patients
Few studies have looked at the makeup of patients that utilize the ED for migraine and why these individuals seek care in the ED. Some research has suggested that migraineurs who use EDs are more likely to be female, older, and non-white. Narcotic use, lower socioeconomic status, and overuse of emergency services have also been linked to ED visits for migraine. In addition, mood disorders may contribute to ED visits for migraine.
Assessing Diagnostics
Imaging practices for migraine in the ED vary widely despite clinical recommendations and guidelines being available to help emergency physicians decide on whether or not to conduct such imaging. Patients presenting to the ED with a recurrence of their baseline headache disorder are not recommended to receive head imaging.
It has been hypothesized that if emergency physicians had more time or resources to reassure patients and educate them about their headache diagnosis, the need for imaging may be diminished. Health information exchange may help decrease use of unnecessary diagnostic imaging and increase use of evidence-based guidelines for evaluating headaches in EDs.
Analyzing Treatment
Many migraine patients report not taking medications—including acetaminophen—before coming to the ED. Most acute migraine treatment recommendations are general in nature and are not specifically aimed at ED settings. Several pharmacologic migraine-specific therapies can be used for managing patients in the ED, but actual practices in the emergency setting differ from current guideline recommendations. More than 20 different medications are commonly used to treat migraine, but triptans—one of the most effective classes of migraine-specific drugs—are rarely used in the ED, according to studies. Furthermore, a large percentage of migraineurs do not receive any pharmacologic treatment at all in the ED.
Opioids are also commonly prescribed for managing migraine, but published reviews recommend against using these therapies because they are not consistently effective and are associated with other risks. “Migraine patients often don’t get recommended migraine-specific medications in the ED and are instead being given opioids, which have risks of abuse and addiction,” says Dr. Minen. “We need a better understanding as to why opioids are still prescribed for migraines in EDs despite recommendations to avoid using these drugs for this reason. Opioids can also render other headache-specific therapies less effective.”
Looking Ahead
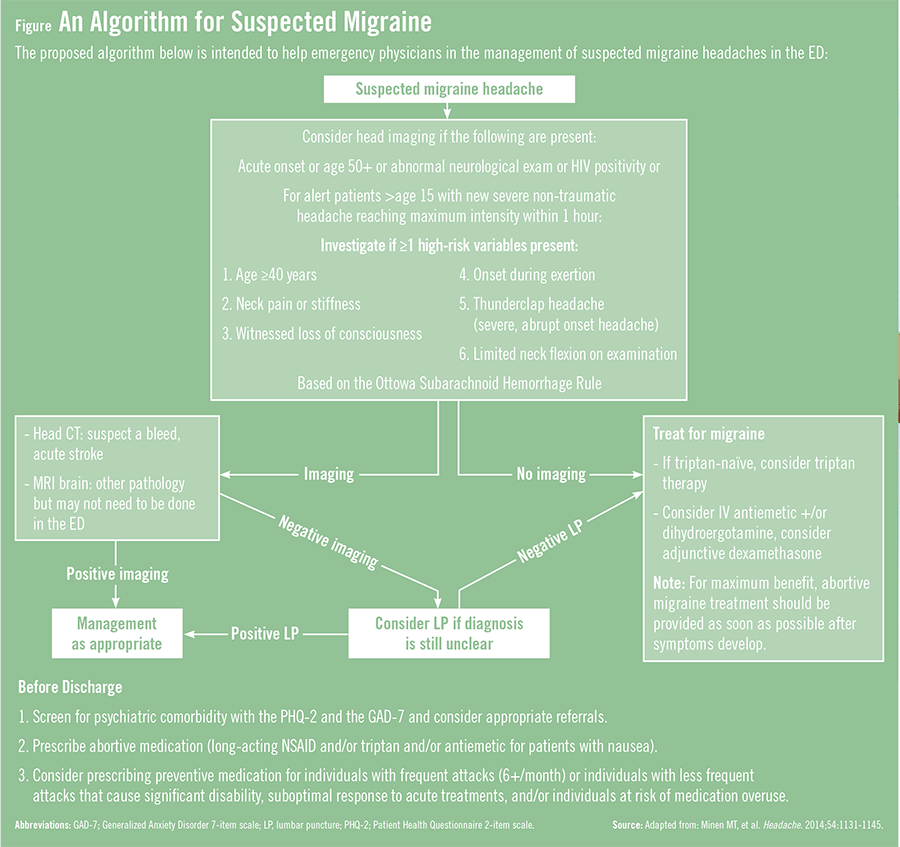
There is currently insufficient evidence to recommend definitive approaches for managing migraine, but Dr. Minen says it is important to develop an algorithm for treating patients in the ED setting. “We need to have an algorithm for migraine like the ones that have been developed for acute coronary syndromes and stroke,” she says. A proposed algorithm (Figure) has been developed to help emergency physicians manage suspected migraine headaches, but more research is needed to determine whether it can improve short- and longer-term outcomes for migraineurs.
Broader studies are also needed to understand the rationale for ordering head imaging so that interventions can then be designed to decrease the use of CTs. In addition, studies suggest that patients often leave EDs without a discharge diagnosis, outpatient medication, or instructions. “To improve the care of migraine in the ED, coordinated efforts are needed from emergency physicians, neurologists, psychiatrists, primary care physicians, and other key constituents,” says Dr. Minen. “This is paramount to ensuring that patients receive optimal work-ups, treatment, and follow-up.”
 TimH
TimH
{kind=link}