
Research has shown that many patients in the United States present to the ED with gastrointestinal (GI) complaints, but these problems can often lead to inefficient and expensive testing. “In many cases, patients come to the ED with abdominal pain that is non-specific,” explains Andrew C. Meltzer, MD. “Even after diagnostic tests are ordered, ED patients are frequently discharged with a diagnosis of non-specific abdominal pain.” In previous studies, investigators have found that there appears to be a link between GI disorders and psychiatric disorders.
The Role of Mental Health
Some researchers have theorized that depression and anxiety can be attributed to many cases of non-specific abdominal pain, but few analyses have explored this association in greater detail. To address this issue, Dr. Meltzer and colleagues had a study published in the Western Journal of Emergency Medicine. The study sought to determine if repeat ED use among patients with non-specific abdominal pain might be associated with a diagnosis of moderate to severe depressive disorder. Identifying patients who may clinically benefit from targeted psychiatric screening may help improve their quality of life and enable clinicians to use diagnostic tests more efficiently.
For the study, 987 ED patients were screened for major depression during weekday daytime hours using the Patient Health Questionnaire-9 (PHQ-9), a depression screening tool that has been validated in previous research. Each study participant was classified as having no depression, mild depression, or moderate-to-severe depression based on their PHQ-9 results. According to the results, about 62% of patients with non-specific abdominal pain who had moderate or severe depression—defined as scoring a 10 or higher on the PHQ-9—had at least one visit to the ED for the same complaint within a 1-year period (Table 1). That percentage dropped to about 29% for patients with non-specific abdominal pain who had no depression, defined as scoring less than 5 on the PHQ-9.
{kind=link}
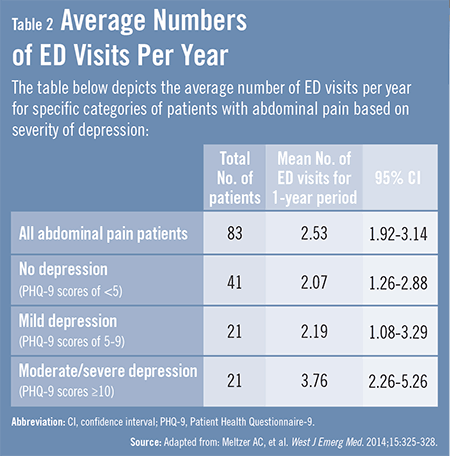
“Our analysis also showed that, on average, patients with non-specific abdominal pain with moderate or severe depression had 3.76 visits per year, compared with 2.19 visits per year for those with abdominal pain and mild depression and 2.07 visits per year if patients had a negative depression screening on the PHQ-9,” says Dr. Meltzer (Table 2). “These findings illustrate the importance of finding new diagnostic and therapeutic strategies to care for these patients.”
{kind=link}
Public Health Implications
According to the study, understanding the association between non-specific abdominal pain, serial ED visits, and depression may have significant public health implications. The observed associations may be due to the fact that patients who return to the ED on multiple occasions are more likely to have a chronic medical condition. In addition, functional GI disorders, such as IBS, dyspepsia, and others, have been shown in studies to be strongly associated with psychiatric disorders like depression and anxiety.
The study team also reported that depressed patients may be less likely than those without depression to have access to healthcare at sites other than EDs. Research shows that EDs are relatively easy healthcare access points when compared with other mental health services. “In general,” Dr. Meltzer says, “depressed patients may be more likely to use the ED for all of their healthcare needs.” As non-specific abdominal pain goes unresolved, patients may repeatedly visit the ED when psychiatric or psychosocial stressors worsen.
Other reasons may also be part of the problem, according to the study. For example, the non-specific abdominal pain that patients experience may be a form of somatization, which occurs when physical symptoms are misattributed to medical rather than psychiatric causes. Known risk factors for somatoform disorders include (among others):
♦ Lower socioeconomic status.
♦ Limited education.
♦ Alcoholism.
♦ Social dysfunction.
Patients with depressive illnesses commonly describe their psychological distress in physical terms. When these patients do not appear to have any emergent medical illness after being examined by a physician, they may be discharged without addressing the psychiatric root of their visit. When psychiatric symptoms go unaddressed, patients may revisit EDs without an appropriate diagnosis.
Looking Forward
“More studies are needed to confirm the associations observed in our study and to determine how best to manage abdominal pain,” says Dr. Meltzer. “In the future, it’s hoped that predictive models will be developed and tested to help clinicians determine which patients are likely visiting the ED repeatedly because of mental illness rather than their non-specific abdominal pain. In the meantime, clinicians should consider depression as a possible cause of this pain. They should also think about screening patients who have visited the ED multiple times for non-specific abdominal pain for depression.”