

Catheter-associated blood stream infections (CABSI) can have a significant impact on patient morbidity while increasing healthcare utilization costs. CABSIs are preventable, and several strategies are used to reduce these infections, including training healthcare workers, ensuring compliance with proper placement technique, promptly removing catheters associated with a high risk of infection or that are no longer needed, and providing feedback to improve healthcare worker accountability. These strategies have focused largely on central venous catheters and ICUs, but few data are available in the non-ICU setting.
Peripheral venous catheters (PVCs) are commonly used in hospitals, but previous studies have reported poor compliance with the care of these catheters and serious events relating to infectious complications. “In many hospitals, there is room for improvement in the maintenance and care of PVCs,” says Mohamad G. Fakih, MD, MPH. “Improving the process will help reduce the risk of CABSI.”
Testing an Intervention to Improve PVC Care
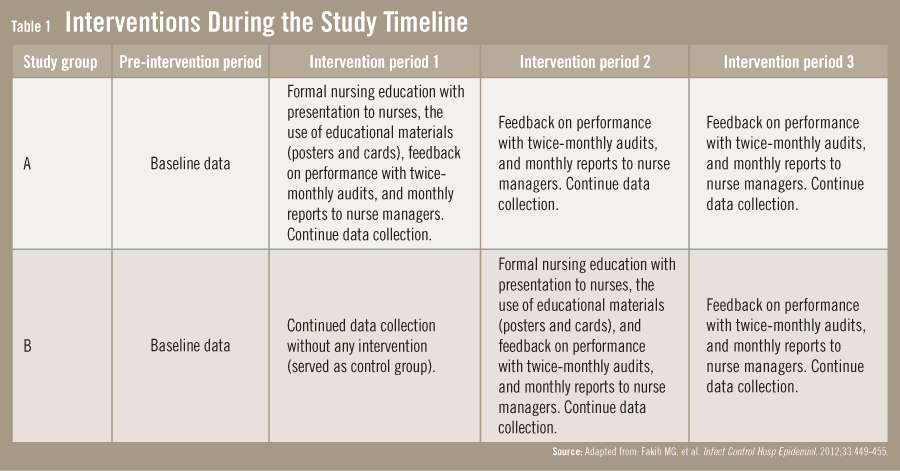
In the May 2012 issue of Infection Control and Hospital Epidemiology, Dr. Fakih and colleagues had a study published evaluating the effect of education and feedback on process measures to improve PVC care and infectious complications. Nurses and patients in 10 non-ICUs were involved in the analysis, and the intervention was applied during four periods, each one lasting 3 months in duration. The four periods included a pre-intervention phase and three staggered real-time education and feedback interventions. “Our study intervention included use of formal lectures, printed educational materials, audits, and immediate feedback to the nurses on their performance,” adds Dr. Fakih.
Five units participated in the intervention (Group A), while the other five served as a control group (Group B) (Table 1). Group B underwent the intervention during intervention period 2, and both Group A and Group B received feedback on performance during intervention period 3. Process measures were evaluated twice monthly, and feedback was given to nurses directly and to the unit manager on a monthly basis.
Reducing Infection Risk from PVC
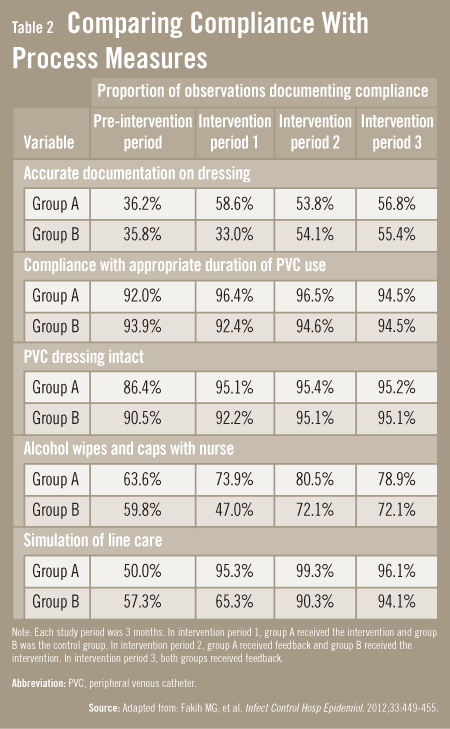
The nurses’ knowledge and performance significantly improved in the intervention Group A, compared to controls (Group B). Similar improvements were seen in Group B when exposed to the intervention. The improvements were also reflected in processes for both groups (Table 2). “Providing education and real-time feedback to nurses increased and sustained compliance with processes aimed at reducing the risk of infection from PVCs,” Dr. Fakih says. “For example, the accurate documentation on dressing increased from 38% before the intervention to 59% after it,” explains Dr. Fakih. “Cases in which catheter dressings were intact rose from 89% to 95%. Importantly, the ability to correctly demonstrate scrubbing the hub before infusion increased from 54% to 95%.” A significant reduction in PVC-associated bloodstream infection was also seen, dropping from 2.2 cases per 10,000 patient-days during the pre-intervention period to 0.44 cases per 10,000 patient-days during the three intervention periods.
Online Exclusive
Table 3: Bloodstream Infection Rates Associated with Different Catheters
In addition to improving overall rates of CABSI, the persistence of marked improvements in process measures was observed throughout the stages of the intervention. A reduction in phlebitis rates was also observed, with rates averaging about 2%, which falls in the lower range of what has been reported in previous studies. Dr. Fakih notes that it may be better to use PVC-associated bloodstream infection rather than phlebitis as an outcome measure when evaluating quality improvement processes for reducing infection risks associated with PVC.
In an evaluation of nurses’ knowledge before and after education, many of the nurses in the study were already familiar with the standards of care for PVC and with the risks for infection. “This suggests that education alone may not be enough for improving processes and outcomes,” says Dr. Fakih. “Other factors should be considered, including nurses’ perception of the potential risk to patients, their manager’s involvement, and whether they view the intervention as being beneficial. Feedback plays an important role in ensuring that educational interventions have a lasting effect.”
Implications for Hospital Intervention
Implementing the educational intervention assessed in Dr. Fakih’s study would likely require buy-in from hospital leaders and staff and a hospital culture that fosters such efforts. There are several actions hospitals should consider taking to improve processes and outcomes related to PVC care, according to Dr. Fakih. “Hospitals should establish a process to enforce compliance with standards of line care. They should also consider intervening in areas associated with a high risk or high prevalence of infections. Providing direct feedback in addition to formal education and establishing a process for periodically assessing the units involved can also be helpful.”
 TimH
TimH
{kind=link}
{kind=link}