
For older Americans, persistent pain is highly prevalent and costly to manage. Persistent pain most often is attributable to musculoskeletal causes, usually involves multiple sites, and typically occurs in the presence of other comorbidities. “As adults in the United States continue to live longer, there is an increasing need for more physician education on the management of persistent pain among older adults,” says Cary Reid, MD, PhD. “Most doctors, however, receive little training on managing pain, especially for older patient groups. Furthermore, many clinical studies examining various drug therapies exclude older patients.”
In a clinical review published in JAMA, Dr. Reid and colleagues examined barriers to persistent pain management among older adults and summarized pharmacologic and non-pharmacologic approaches for this patient population. The article also provided information on rehabilitative modalities that are important to consider and highlighted aspects of the patient-physician relationship that can help to improve outcomes. “This information is important as efforts are increasing to use age-appropriate approaches to delivering pain care for older adults,” says Dr. Reid.
Potential Barriers
There are several important barriers to managing persistent pain in the geriatric population. Some examples include age-related physiologic changes that alter drug absorption, sensory and cognitive impairments, polypharmacy, and multiple comorbidities. “There is also limited evidence to help guide pain management in older patients,” adds Dr. Reid. “In addition, older adults have varying beliefs about pain and when it requires treatment.” In addition, many physicians have concerns about the potential for treatment-related harm that can result from using pain medications in these patients, which causes them not to treat pain further and further compounds the problem.
Multimodal Approaches
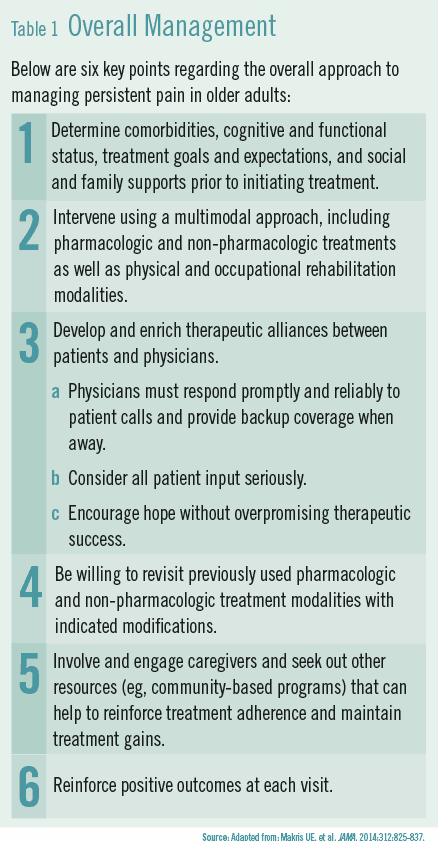
According to Dr. Reid, it is important for physicians to use a multimodal approach to managing persistent pain in their older patients. “There should be an emphasis on combining both pharmacologic and non-pharmacologic treatments rather than focusing on one or the other,” he says (Table 1). “It’s important to include physical and occupational rehabilitation as well as cognitive-behavioral therapy and movement-based interventions. Unfortunately, research indicates that these treatments are largely underutilized.”
Ideally, an integrated approach will cultivate a strong therapeutic alliance between older patients and their physicians. Dr. Reid says that using a collaborative care strategy is paramount to formulating an effective treatment plan for older patients with persistent pain. “This requires a clear understanding of patients’ comorbidities, cognitive and functional status, and treatment goals and expectations,” he says. It also requires a review of patients’ resources, including both social and family support networks.
A Stepwise Approach
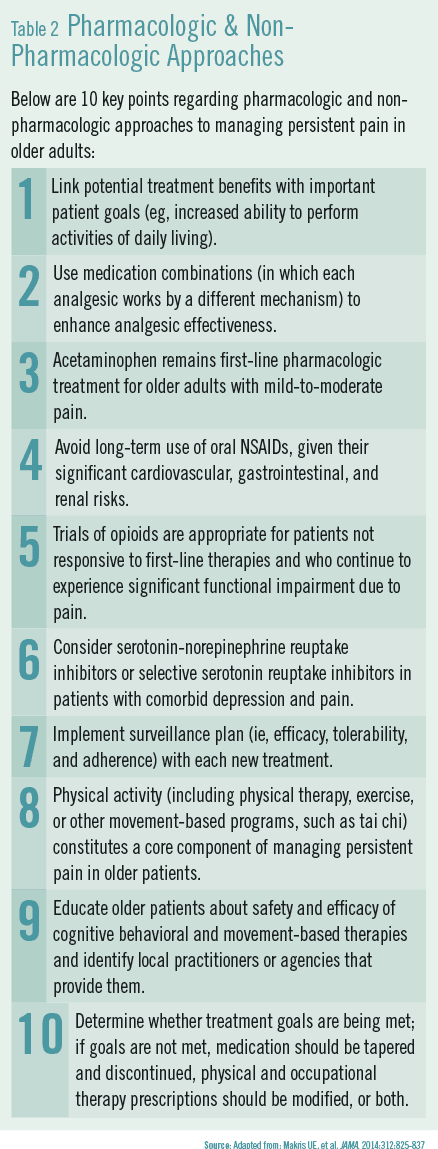
The article in JAMA recommends using a stepwise approach to managing persistent pain (Table 2). Careful surveillance to monitor for toxicity and efficacy is critical because advancing age increase the risk of adverse effects. Research shows that acetaminophen is typically beneficial as first-line therapy, but a trial of a topical NSAID, tramadol, or both is recommended if treatment goals are not met. Oral NSAIDs are not recommended for long-term use in older patients.
Physicians are recommended to start at the lowest possible dose of pain medication and titrate up based on tolerability and efficacy. Use of two or more analgesic drugs with complementary mechanisms of action—as opposed to higher doses of a single pain medication—may lead to greater pain relief with less toxicity.
Dr. Reid says it is important to consider referring older adults with persistent pain to specific non-pharmacologic modalities that are both accessible and affordable. “Physicians should make efforts to find physical therapy and occupational therapy services for older patients,” he says. “We should encourage the use of non-pharmacologic approaches and engage the patient’s family and caregivers in these efforts. These efforts can help cultivate and reinforce a long-lasting therapeutic alliance that is based on trust, which in turn makes it possible to improve outcomes for patients over the long term.”
Looking Forward
In the future, Dr. Reid says mobile health technology and other interventions are likely to further improve how older patients with persistent pain are managed. “As technology continues to evolve and new interventions emerge,” he says, “there is hope that we’ll be able to enhance our care of older patients in a cost-effective and convenient manner.” He notes that early data suggest that older patients are willing to use mobile technologies to help manage their pain and adds that the need for more skilled professionals to provide non-pharmacologic treatments is likely to increase. “In the meantime,” he says, “physicians should consult established clinical guidelines and make treating persistent pain a greater priority so that older adults can have the best quality of life possible.”
 Janine Anthes
Janine Anthes
{kind=link}
{kind=link}