
The quality of care coordination is important to the United States healthcare system as hospital readmission rates are being further scrutinized. When hospital readmission rates are high, it is often the result of poorly coordinated care across the full continuum of care settings, from EDs and ICUs to primary care and outpatient settings. As care is better coordinated, it is more likely that these rates will be reduced. “Improving the coordination of care for patients is also important to Medicare and to hospitals,” says David C. Goodman, MD, MS. “Medicare patients who return to hospitals shortly after they’ve been discharged add substantial costs to Medicare that could be avoided with better post-discharge care.”
CMS estimates that the cost of avoidable readmissions is more than $17 billion per year. In the coming months, there are plans in place to reduce Medicare payments for readmissions if hospitals have higher-than-expected 30-day readmission rates for patients with acute myocardial infarction (AMI), congestive heart failure (CHF), or pneumonia. In 2013, hospitals face a penalty equal to 1% of their total Medicare billings if an excessive number of patients are readmitted. The penalty rises to 2% in 2014 and 3% in 2015.
Hospitals Currently Struggling
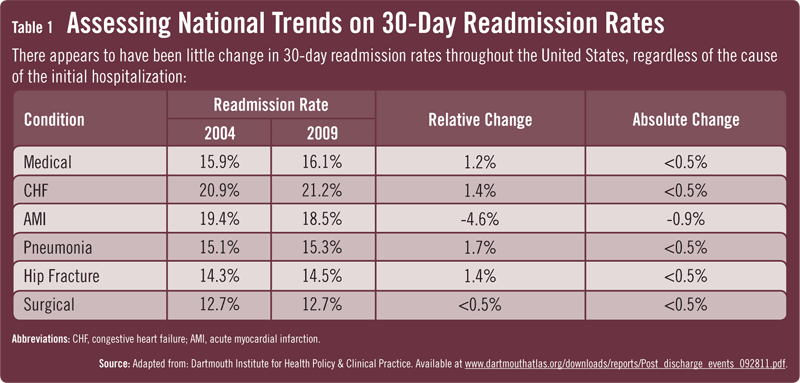
In September 2011, the Dartmouth Institute for Health Policy & Clinical Practice released the Dartmouth Atlas report, which analyzed readmission rates among Medicare patients for AMI, CHF, pneumonia, and other hospital discharges between 2003 and 2009. Researchers examined the records of 10.7 million Medicare patient hospital discharges and found little progress during the study period. Patients hospitalized for CHF, pneumonia, surgery, hip fractures, or other medical conditions had 2009 readmission rates that were either the same or slightly higher than those observed in 2003 (Table 1). About 20.9% of patients with CHF returned to the hospital within 30 days in 2004, but the rate increased to 21.2% in 2009, the highest readmission rate observed in the analysis. Improvement was observed in readmissions for AMI within 1 month of discharge, decreasing from 19.4% in 2004 to 18.5% in 2009.
The goal should be to ensure that patients are receiving quality care that minimizes the risk of preventable readmissions.
“The Dartmouth Atlas report was the first to look at how effectively communities and hospitals coordinate care for some of their sickest patients— those who leave the hospital after staying for treatment of an acute or chronic illness,” explains Dr. Goodman, who was the co-principal investigator of the report. “The report highlights widespread and systematic failures in coordinating care. Unnecessary hospital readmissions can lead to more tests and treatments for patients as well as higher healthcare costs and utilization, regardless of the cause of readmission.”
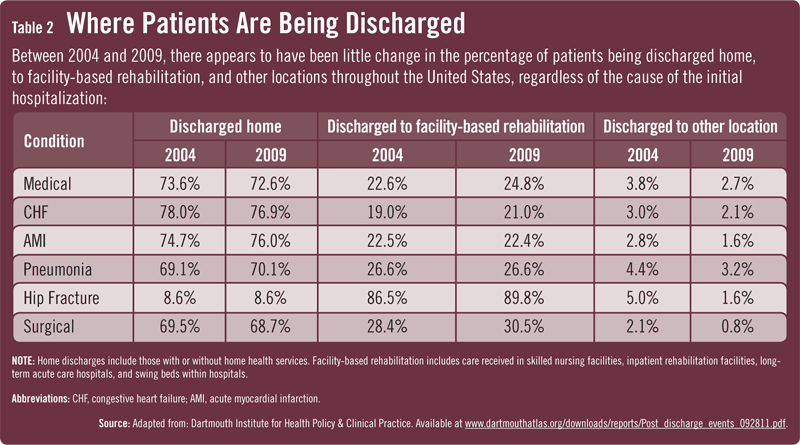
The report also assessed the frequency of clinician follow-up visits within 14 days after patients were discharged from the hospital. The outpatient patterns demonstrated serious and persistent gaps in care coordination after hospital discharge (Table 2). In only a few regions of the U.S. did more than half of patients see a primary care clinician within 2 weeks of leaving the hospital; in many regions, less than half saw any clinician after being discharged. “There is clearly a need to develop more efficient systems of care that include discharge planning and care coordination,” adds Dr. Goodman.
A Wake-Up Call
The Dartmouth Atlas report illustrates that there is opportunity for improvement. It also highlights the importance of striving to reduce readmissions with other policy and payment initiatives. “The findings should serve as a wake-up call to all constituents who are concerned with high readmission rates,” says Dr. Goodman. “They underscore the need for hospitals, patients, and outpatient and inpatient providers to collaborate in a coordinated fashion. The goal should be to ensure that patients are receiving quality care that minimizes the risk of preventable readmissions.”
Most efforts to reduce readmission rates have focused on specific processes of care, but an equally important factor associated with higher rates in the Dartmouth Atlas was the overall intensity of inpatient care that was provided to patients within a region or hospital. “In general, places with patterns of relatively high use of hospitals for medical conditions were oftentimes the same places with high readmission rates,” Dr. Goodman notes. “As such, improving care for older patients will require us to pay attention to the overall systems of care in communities, including the supply of inpatient and outpatient resources. For many patients, episodes of care have no definite end. As we make strides toward improving care coordination, greater efforts will also be needed to develop lifelong models of longitudinal care.”
 Janine Anthes
Janine Anthes
{kind=link}
{kind=link}