
According to published data, Clostridium difficile infection (CDI) now rivals MRSA as the most common organism to cause healthcare-associated infections (HAIs) in the United States. The proportion of hospital discharges in which patients received a diagnostic code for CDI more than doubled between 2000 and 2003, and rates continued to increase in 2004 and 2005. “In addition to increased frequency of CDI, current research also shows that these infections are increasing in severity,” says Erik R. Dubberke, MD.
CDI has been associated with increased lengths of hospital stay, higher costs, and greater morbidity and mortality. According to study data, CDI has been shown to increase lengths of hospital stay by about 3 days. Costs have also been significant; the total U.S. hospital costs for CDI management have been estimated at about $3.2 billion per year. The infection has been associated with attributable mortality rates of 16.7% at 1 year.
New Guidance
In 2008, a task force to create a concise compendium of recommendations for the prevention of common HAIs was appointed by the Society for Healthcare Epidemiology of America and the Infectious Diseases Society of America. Recommendations were published in the October 2008 supplement to Infection Control and Hospital Epidemiology and are available at www.preventingHAIs.com. The document is designed to help hospitals focus and prioritize their efforts to implement evidence-based practices for the prevention of HAIs, including CDI.

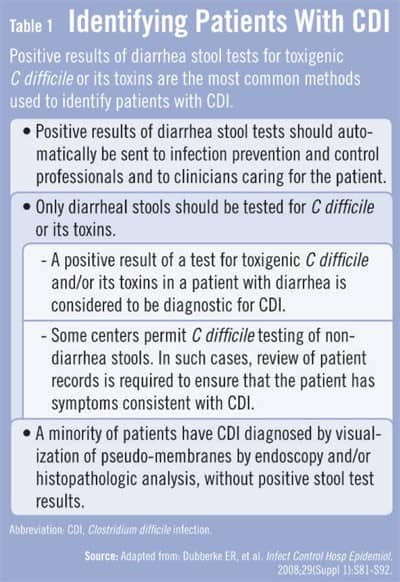
According to the compendium recommendations, fluoroquinolones had been infrequently associated with CDI. However, new research has found that these agents are one of the primary predisposing antimicrobials associated with the infection. “Most antibiotics have been associated with CDI,” explains Dr. Dubberke. “It’s important to consider patient characteristics that may be risk factors for CDI. The detection of CDI can be challenging for clinicians.” The recommendations note that the most commonly used methods for identifying the infection are positive results from diarrhea stool tests for toxigenic C difficile or its toxins (Figure 1).
Prevention Strategies
There are two primary strategies to preventing CDIs that have been outlined by previously published guidelines. The first is to implement strategies that reduce the risk of CDI if the organism is encountered by patients. In these circumstances, clinicians should restrict the use of antimicrobial therapies and implement stewardship guidelines. The second involves using strategies that prevent patients from being exposed to C difficile (Figure 2). “Understanding the importance of disinfection and barrier methods is critical to preventing CDI,” Dr. Dubberke says. “One area of frequent confusion is the preferred method of hand hygiene after caring for patients with CDI. Although alcohol does not kill C difficile spores, no studies have identified an increase in CDI with alcohol-based hand hygiene products. In addition, alcohol-based products are associated with better compliance and are superior at preventing the spread of other organisms.”
Besides hand hygiene, Dr. Dubberke says that physicians managing CDI must wear gloves and gowns prior to entering patients’ rooms. “Hands are just as likely to be contaminated with C difficile even if there is no direct patient contact,” he adds. “However, proper hand hygiene is still important even after glove removal. Furthermore, hospitals and their staff must monitor housekeeping protocols. Diluted bleach appears to be effective only in areas experiencing a CDI outbreak. The key is for institutions to establish processes and protocols that everyone on staff will practice routinely.”
The compendium recommendations also describe other important principles that clinicians should be aware of when caring for patients with CDI. For example, testing for C difficile should only be performed on unformed diarrhea stools; toxin testing of formed stool is strongly discouraged. Prophylactic antimicrobial CDI therapy should not be given to patients at high risk for CDI. Additionally, attempts to decolonize asymptomatic C difficile carriers should not be carried out, and antimicrobial therapy is not effective for decolonization. The recommendations also note that repeated testing for C difficile should not be performed if patients have had a stool sample test positive for the organism unless symptoms resolved with treatment and then returned after treatment.
Get on Board
An important step to preventing CDI is to educate healthcare personnel and hospital administration about the clinical features, transmission, and epidemiology of CDI. “Process measures are a core component for hospitals to be accredited,” says Dr. Dubberke. “Administration must be on board and provide the resources needed for an effective antimicrobial stewardship and other infectious disease and safety services. There may be added costs to consider, but preventing even a handful of C difficile cases can more than make up for the costs for doing surveillance and initiating protocols.”
 JonN
JonN
{kind=link}
{kind=link}