
Renal artery stenosis (RAS)—narrowing of the renal arteries—is often asymptomatic, but studies show that it may lead to hypertension or worsening of blood pressure (BP) control. If left untreated, RAS can cause kidney failure and heart failure. “Optimal medical therapy is the preferred first-line treatment, but many patients who fail medical therapy may benefit from angioplasty and stenting,” explains Sahil A. Parikh, MD, FACC, FSCAI. “These treatments help to reduce the clinical consequences of RAS.” Studies show that more than 90% of RAS cases result from atherosclerosis, yet there is still debate among experts on the role of medical therapy versus revascularization.
Renal artery stenting has emerged as an important primary revascularization strategy in most patients with atherosclerotic RAS. Stenting has become the preferred endovascular technique to manage RAS, with recent studies showing such procedures improve systolic and diastolic BP with excellent safety profiles. However, many of these analyses have non-randomized trial designs, and others excluded some patients who may benefit from renal stenting when randomized trials were conducted. The clinical data have resulted in less widespread acceptance of the benefits of renal artery stenting.
New Guidance on Renal Artery Stenting
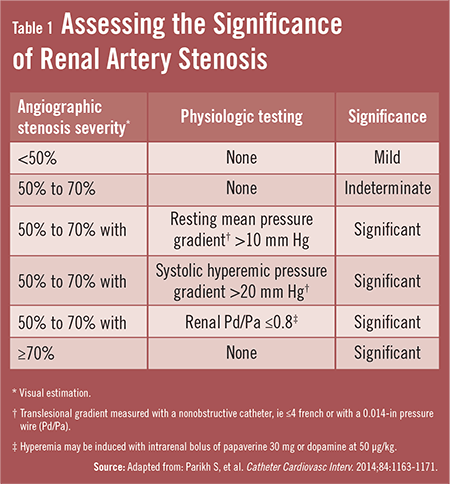
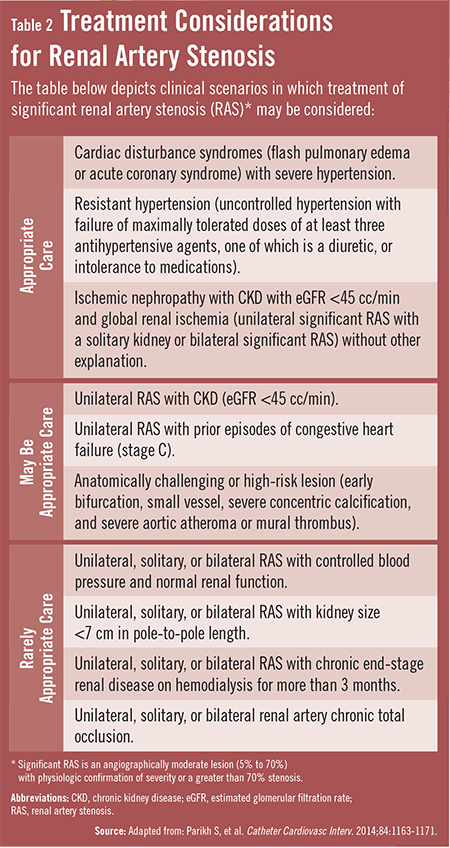
In 2014, the Society for Cardiovascular Angiography and Interventions (SCAI) released a new expert consensus statement for the appropriate use of renal artery stenting. The document, which was based on an expert panel review of scientific data, was developed to help guide physicians in applying renal stenting. SCAI also highlights the current limitations in the peer-reviewed literature and identifies opportunities to advance the field. The consensus statement offers clinicians measures to assess the significance of RAS (Table 1) as well as clinical scenarios in which treatment of significant RAS may be considered. The clinical scenarios are divided into cases in which care is appropriate, may be appropriate, and is rarely appropriate (Table 2).
“A key component of the consensus statement was that it incorporated data from the Cardiovascular Outcomes in Renal Atherosclerotic Lesions (CORAL) trial, which was a prospective, multicenter randomized study that took about 10 years to complete,” says Dr. Parikh, who was on the SCAI writing group that developed the document. The CORAL trial, in addition to other similar investigations, failed to demonstrate a benefit of renal stenting over optimal medical therapy. However, there were patients who may have had better outcomes with renal artery stenting who were excluded from these trials.
“The CORAL trial answered many questions about renal artery stenting for patients with RAS,” Dr. Parikh says. “However, some patients who are seeking this treatment today were not included in CORAL, including some in whom optimal medical therapy failed. The new recommendations were developed to help physicians evaluate the available treatment options for a broad range of patients with RAS.”
What Patients Can Benefit?
The SCAI consensus statement notes that several groups of patients are most likely to benefit from renal artery stenting. These patients include those with cardiac disturbance syndrome or “flash” pulmonary edema, those whose hypertension has not been controlled by three or more medications at maximal tolerated doses, and those with blockages in both kidneys or severe blockages in a single functioning kidney where BP or renal dysfunction cannot be managed medically. The SCAI expert panel also identified poor candidates for renal artery stenting procedures. These included patients with:
♦ Mild or moderate blockages (less than 70%).
♦ Long-standing loss of blood flow.
♦ Complete blockages of the renal arteries.
Studies show that these individuals are typically not good candidates for renal artery stenting. The consensus document noted that it is unknown if renal artery stenting can yield long-term improvement of symptoms in patients with heart failure.
In addition, the SCAI expert consensus document reviewed the expert opinion and evidence on the performance of renal artery angiography and interventions with stents. The panel indicated that while narrowing of more than 70% in severity is usually significant, those with intermediate narrowing—50% to 70%—require additional testing with hemodynamic pressure gradient measurements to determine if a lesion is clinically important.
Opportunities Remain on Renal Artery Stenosis
“Most physicians performing renal artery stenting procedures will find that the guidance from SCAI is particularly helpful for assessing RAS in the future,” says Dr. Parikh. “The CORAL trial and others have added to our understanding of the pathophysiology of RAS and the role of renal artery stenting. However, as our understanding of RAS and its treatment options grows, there is hope that physicians will enhance their ability to improve symptoms and quality of life for more patients.”
 TimH
TimH
{kind=link}
{kind=link}