

The Occluded Artery Trial (OAT) was a large, randomized controlled study funded by the National Heart, Lung, and Blood Institute that tested routine percutaneous recanalization of persistently totally occluded infarct-related arteries identified a minimum of 24 hours after myocardial infarction (MI) in stable patients who did not have triple vessel disease or severe inducible ischemia. In 2006, results from OAT were released, showing that there appears to be no benefit to routinely using PCI for persistently totally occluded infarct-related arteries in this patient population. Routine PCI for these arteries did not reduce mortality, reinfarction, or class IV heart failure. These results subsequently led to updates of guidelines from the American College of Cardiology (ACC) and American Heart Association (AHA) on unstable angina/non-STEMI, STEMI, and PCI in 2007. The revised guidelines recommended that PCI not be performed in this context.
Prior to OAT data being released, clinicians tended to favor using PCI for persistent infarct-related artery occlusions largely because of experimental and observational data. “OAT results demonstrated that use of PCI did not lead to a reduction in clinical events,” explains Judith S. Hochman, MD. “The beneficial effect on angina and quality of life was small and not durable. OAT also suggested that PCI was more costly than optimal medical therapy alone. As a result, these findings should have discouraged routine PCI in this setting.”
Assessing the Impact of the OAT Study In the October 10, 2011 Archives of Internal Medicine, Dr. Hochman and colleagues had a study published in which they examined whether PCI use for treating occluded infarct-related arteries after an MI decreased following the publication of OAT results and the resultant updates to the ACC/AHA STEMI and NSTEMI guidelines. “It’s important to measure the degree to which clinical trials and guidelines affect cardiology practices in the United States,” says Dr. Hochman.
Using data from the National Cardiovascular Data Registry and its CathPCI Registry, they analyzed the hospital visits of 28,780 patients in the United States who underwent angiography at least 24 hours after an MI over a 3-year period. The study timeframe allowed the research team to examine data before OAT results and ACC/AHA guidelines were released and the resulting effect after these documents were published.
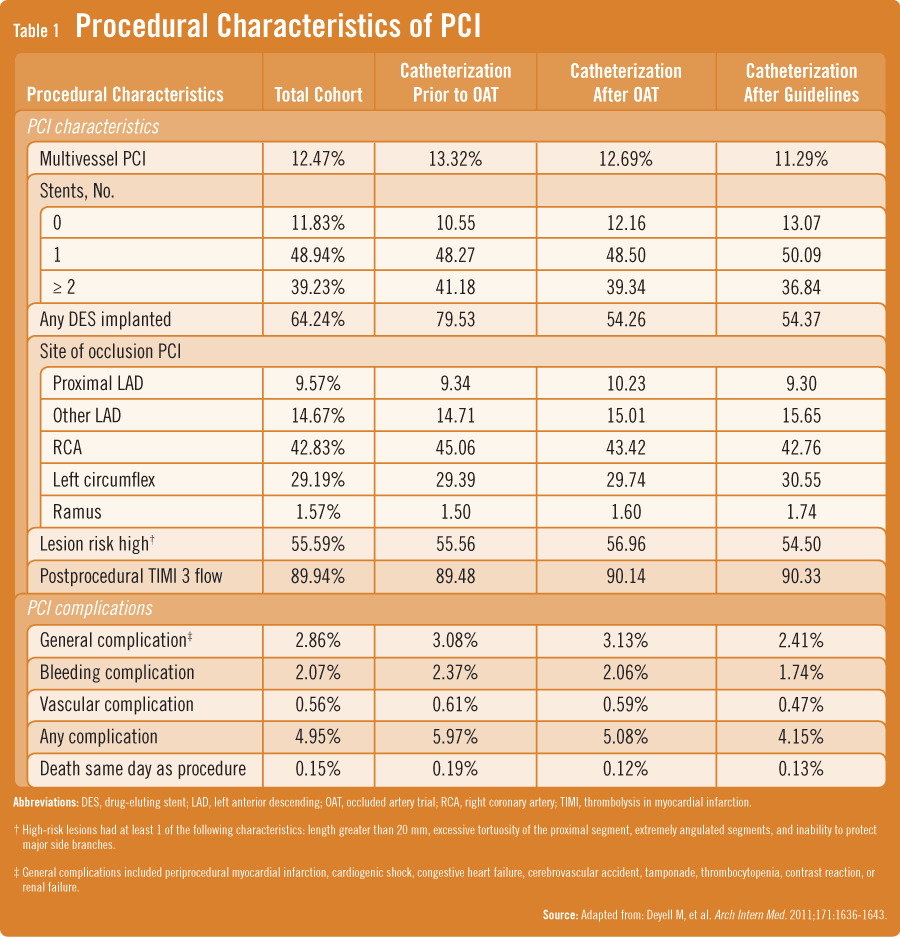
According to the study findings, there appeared to be no overall change in the adjusted rate of PCI use for total occlusions after an MI following publication of OAT and the STEMI and NSTEMI guidelines (Table 1). “During 2 years of follow-up after OAT and 1 year of follow-up after the guideline updates, a considerable proportion of patients in this setting still underwent these procedures despite evidence showing that the approach is not recommended,” Dr. Hochman says. “It appears that the current evidence on PCI for totally occluded infarct-related arteries late after MI in stable patients has not been widely incorporated into clinical practice.”
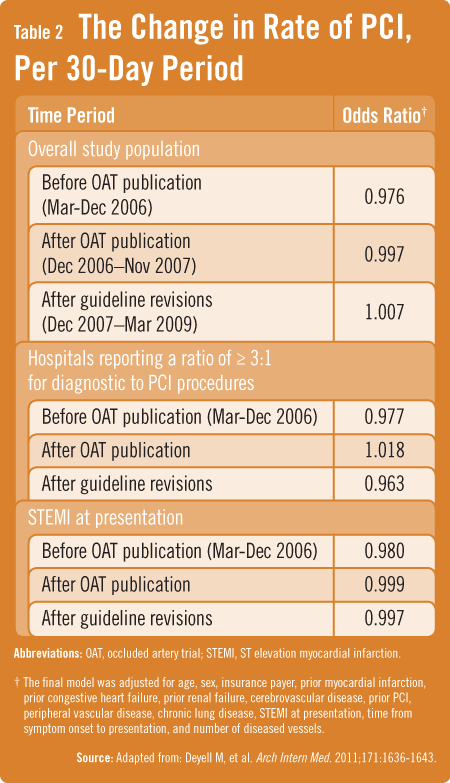
Overall, patients presenting with STEMI and NSTEMI were equally likely to undergo PCI for an occlusion (53.5% vs 53.0%). Among a subgroup of patients presenting with STEMI, there was no difference in the adjusted monthly rate of PCI for occlusions after publication of OAT or after the ACC/AHA guideline revisions from 2007 (Table 2).
A Cause for Concern
Cardiologists and interventionalists have historically incorporated results from positive trials and related guideline recommendations quickly, according to Dr. Hochman. “Unfortunately, results from our analysis indicate that physicians may be less likely to make clinical practice changes. The reasons for the lack of impact that this ACC/AHA guideline recommendation had on clinical practice are likely multifactorial.”
One reason may be due to the negative study results that emerged from OAT. Although OAT was a negative trial overall, it did not suggest excessive harm from PCI aside from a trend toward increased reinfarction. That said, physicians may still be reluctant to alter their practices based on negative results, especially if competing factors are present or if new practices contradict long-held beliefs. Patient expectations and financial incentives may also play a role.
Further Research on Guideline Adoption Warranted
Dr. Hochman says that more research is needed to better understand barriers that prevent physicians from adopting clinical practice guidelines more consistently. “Regardless of the reasons for our findings, clinicians should recognize that many stable patients with totally occluded infarct-related arteries continue to undergo PCI, a costly procedure that did not improve clinical outcomes in this context, despite little evidence to support its use and clinical practice guidelines recommending against it. It’s important to increase awareness of the guideline recommendations for these patients and to promote better adherence to national guidelines on STEMI and NSTEMI.”
 Janine Anthes
Janine Anthes
{kind=link}
{kind=link}