

Research indicates that nearly 90% of new HIV infections in the United States in 2010 were attributed to sexual transmission. However, nationally representative data on sexual risk behaviors have not been available since the late 1990s. Collecting national data on the sexual risk behaviors of people with HIV who are receiving medical care can help clinicians identify those who are at greatest risk of transmitting the virus. It can also help inform prevention efforts to reduce sexual transmission of HIV and the acquisition of other sexually transmitted infections (STIs).
Taking a Closer Look
For a study published in AIDS, Christine L. Mattson, PhD, and colleagues sought to describe sexual risk behavior in a national sample of HIV-infected adults receiving medical care in the U.S. Some patients were virally suppressed—defined as all viral load measurements during the past 12 months less than 200 copies/ml—and some were not. “Given the increased probability of HIV transmission when individuals are not virally suppressed, we also assessed the association between sexual risk behavior and viral suppression,” says Dr. Mattson. “Using interview and medical record data from 2009, we looked at self-reported sexual behaviors in the past 12 months.”
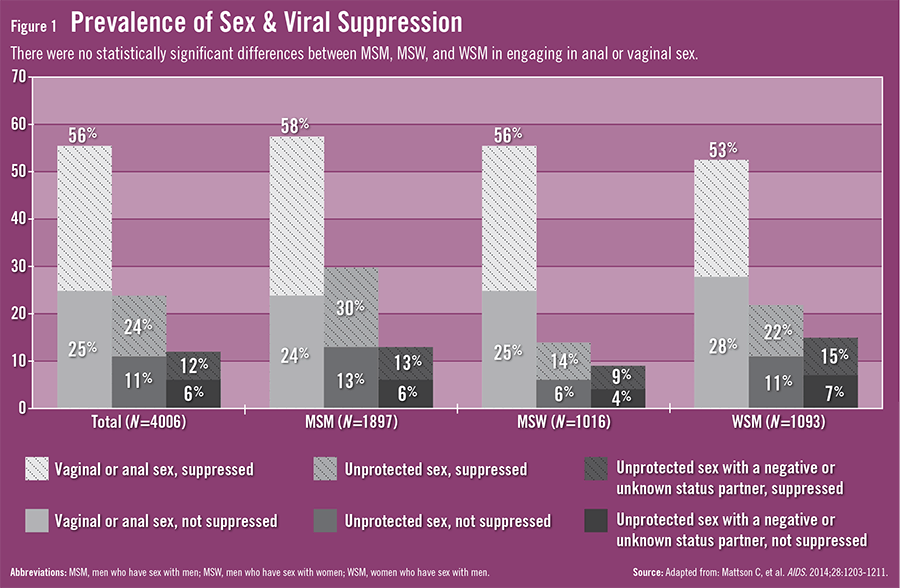
Overall, 56% of participants reported anal or vaginal sex with one or more partners in the past 12 months, 13% reported an STI, and 56% reported not having been tested for STIs. Also, 24% drank alcohol and 11% used drugs before or during sex. Nearly equal percentages of men who have sex with men (MSM), men who have sex with women (MSW), and women who have sex with men (WSM) engaged in vaginal or anal sex (Figure 1). However, there were some differences across risk behaviors. For example, MSM had more sex without a condom than MSW and WSM, and WSM had more sex without a condom than MSW. Also, more WSM had sex without a condom with an HIV-negative or unknown status partner when compared with MSW. “The increased prevalence of risk behaviors among MSM, combined with the increased per-act transmissibility of HIV through anal intercourse, highlights the need for effective prevention efforts for this population,” says Dr. Mattson.

Dr. Mattson emphasizes that the majority of participants (76%) did not engage in vaginal or anal sex without a condom. “That said, 12% did engage in these behaviors with a partner who was HIV-negative or whose HIV infection status was unknown,” explains Dr. Mattson. “Of this 12%, half had viral loads that were high enough to suggest an increased risk of transmission, whereas the other half were virally suppressed, suggesting a reduced risk of transmitting HIV.”
The Effect of ART Use
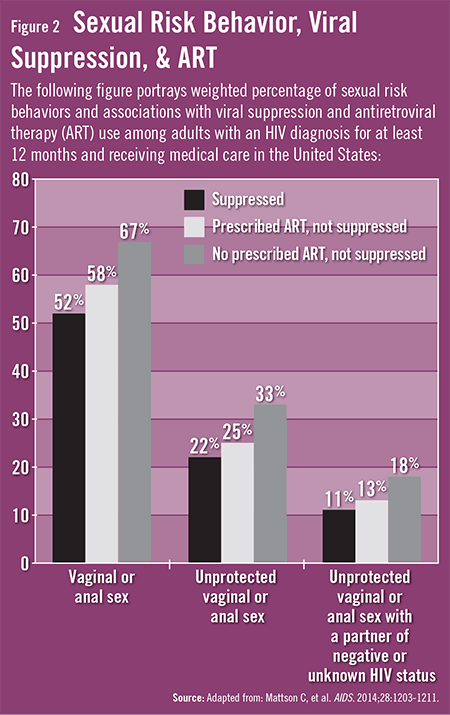
The authors noted that they found no evidence suggesting that patients on antiretroviral therapy (ART) engaged in higher levels of sexual risk behavior than those who were not (Figure 2). This finding is important considering recent concerns that patients who take ART might engage in more risky sexual behavior, regardless of their viral status. “Our analysis showed that patients who received ART were less likely to engage in vaginal or anal sex at all or without a condom with a partner whose HIV status is either negative or unknown,” adds Dr. Mattson.
The data also showed that patients who were prescribed ART were less likely to engage in behaviors that have the potential to transmit HIV, regardless of viral suppression. “This finding suggests that ART use is associated with lower sexual risk behaviors irrespective of viral suppression,” Dr. Mattson says. According to the investigators, this finding may be the result of prevention interventions delivered in the care setting, possible ART side effects (eg, depression or anxiety) that may decrease libido, or an indication that patients who are prescribed ART differ from those who are not.
Important Implications
The study highlights the need to make combination prevention approaches—including behavioral risk reduction, counseling, and access to ART and medical care—available to all HIV-infected adults. “Doing so will help maximize individual and public health benefits,” says Dr. Mattson. “Medical visits provide an opportunity to discuss risk behaviors and reinforce prevention messages that are designed to reduce ongoing HIV transmission to a patient’s sex partners. It also allows clinicians to diagnose and treat STIs and emphasize medication adherence.”
Effective, evidence-based interventions, like Partnership for Health, can be delivered by providers as brief messages during clinic visits, according to Dr. Mattson. “Too few providers discuss HIV prevention with their patients,” she says. “Combination prevention approaches require additional efforts to engage and retain HIV-infected patients in care and improve the delivery of risk reduction interventions in clinical settings.”
 TimH
TimH
{kind=link}
{kind=link}