

Numerous studies have demonstrated that 30-day postoperative complications resulting from unintended harm adversely affect patients and their families and increase institutional healthcare costs. Several medical societies and associations have developed simple, inexpensive surgical checklists to help reduce postoperative morbidity and mortality. These readily available checklists are capable of shifting the hierarchical culture of the operating room (OR). Although there is evidence that these tools enhance communication and reduce postoperative complications and death, studies suggest they are not used universally.
In April 2010, the Association of Perioperative Registered Nurses (AORN) unveiled a comprehensive surgical checklist that incorporates mandated clinical practices required by the World Health Organization, the Joint Commission, and CMS. The one-page document compartmentalizes information to make documentation during the perioperative process easier. It also includes a debriefing component that encourages the OR team to acknowledge concerns and the plan of care for patients to ensure they are safely transitioned to recovery room staff.
Taking a Closer Look
In the Journal of the American College of Surgeons, Lindsay A. Bliss, MD, and colleagues had a study published that sought to determine if combining a structured, team communications training curriculum with a comprehensive, standardized surgical checklist could reduce 30-day morbidity for patients. The communications training included three 60-minute sessions, with topics such as differences between introverts and extroverts, effective dialogue among all OR personnel, and how to use the AORN’s surgical checklist.
High-risk procedures included in the National Surgical Quality Improvement Program database were analyzed for postoperative morbidity. These operations served as the baseline group because the teams carrying out these procedures did not participate in communications training or use a checklist. These surgeries were compared with two other groups. One group included 246 procedures in which surgical teams had undergone communications training. The other involved 73 procedures in which surgical teams had received the same communications training but also used the AORN checklist.
Combined Approach Pays Off
According to results, patients experienced fewer adverse events when they were treated by surgical teams that completed communications training and utilized the AORN checklist before, during, and after high-risk operations (Figure 1). Slightly more than 8% of procedures resulted in complications within 30 days when surgical teams used both the communications training and the checklist. This rate compared favorably to that of surgical teams participating only in communications training (16%) and that of teams who had no communications training and did not use the checklist (23%).
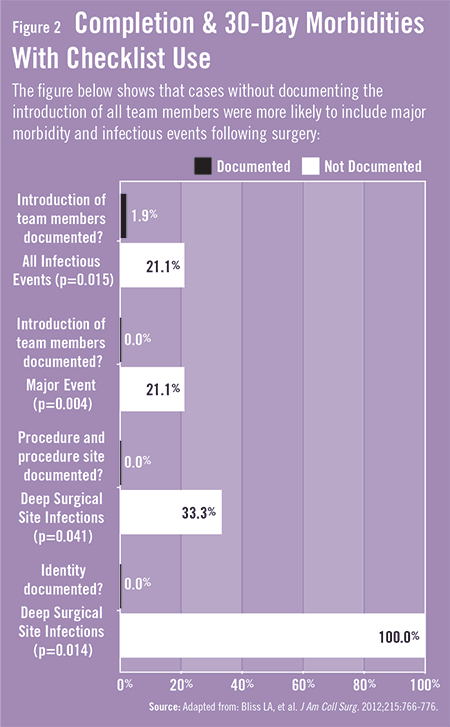
“Even small steps, such as making sure everyone on the team introduced themselves before the surgery, helped reduce complications,” adds Dr. Bliss (Figure 2). “It’s likely that these introductions brought a greater sense of accountability to the team members and ensured that everyone’s voice could and would be heard.” She says that engaging team members in a collegial framework, together with using a surgical checklist, helped to establish plans of care to ensure proper perioperative handoffs and to prepare for and anticipate potential adverse events or complications.
Significant Implications
Having all OR team members understand plans of care can reduce operative time and cost while improving safety and efficiency, Dr. Bliss says. “These findings are important because they help eliminate blame, carelessness, and lack of accountability in the OR. Ultimately, using communications training together with a surgical checklist creates a culture where personnel can be patient advocates without fear of retribution.”
The study builds on previous research about the benefits of using checklists, but also provides other valuable insights. “The implications are significant because payers are now starting to decline reimbursement for complications resulting from errors within 30 days of a procedure,” explains Dr. Bliss. “By taking measures to decrease postoperative complications, we can reduce costs while simultaneously improving outcomes.”
Using the communication training intervention together with a surgical checklist may add a few extra minutes during procedures, but Dr. Bliss says such efforts are worthwhile. “Surgical checklists are available for free online. With more research, it’s possible these tools can be shortened in the future to ensure better long-term compliance. In the meantime, these resources represent cost-effective tools that can reduce postoperative 30-day morbidity and help foster an institutional culture of safety.”
 admin
admin
{kind=link}
{kind=link}