

Research indicates that the adoption of transradial angiography increased 10-fold between 2007 and 2011 in the United States. Randomized and observational studies have suggested that radial access reduces bleeding and vascular complication risks. Other studies have shown the approach reduces costs, increases patient satisfaction, and reduces mortality in some high-risk patients.
3 Major Recommendations
To provide a guide to operators who are early in their adoption of radial procedures or are contemplating adoption, the Society for Cardiovascular Angiography and Intervention (SCAI) published a consensus statement in Catheterization and Cardiovascular Interventions. The document issued three major recommendations:
1. Preserve the radial artery and utilize practices that preserve radial artery patency.
2. Minimize patient and operator radiation exposure during radial procedures.
3. Transradial primary PCI for patients with STEMI should be performed only after sufficient experience is achieved in elective cases.
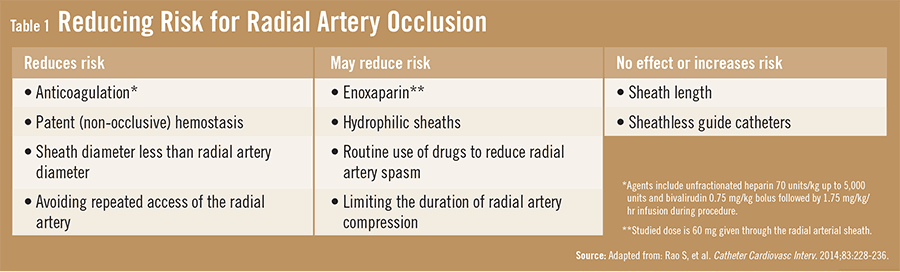
“To monitor for and reduce the risk of radial artery occlusion, we recommend using adequate anticoagulation, the smallest profile equipment possible to minimize trauma to the radial artery and still obtain high-quality images, and non-occlusive hemostasis at the end of the procedure,” says Sunil V. Rao, MD, FSCAI, who served as lead author of the SCAI consensus statement (Table 1). “It’s important to keep enough pressure on the radial artery to obtain hemostasis but not so much that the antegrade flow is prevented.”
The consensus statement also recommends that operators monitor for radial artery occlusions immediately after a radial procedure and during follow-up. SCAI recommends using ultrasound Doppler measurements or the reverse Barbeau test to accomplish this task.
Radiation: Operator Considerations
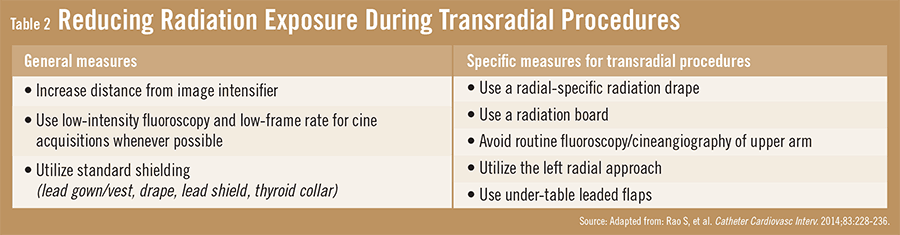
SCAI has published much information on reducing patient and operator radiation exposure during angiography in general. It recommends using radiation shielding, minimizing the use of cineangiography, and relying heavily on fluoroscopic-saving techniques. However, the radial approach necessitates additional, unique approaches (Table 2). “These include positioning the patient’s arm by their side during the procedure as opposed to having it stick out,” explains Dr. Rao. “In addition, clinicians need to become proficient in performing these procedures so that they can be done safely and quickly. We also want to avoid fluoroscopically tracking the guidewire and/or catheters while traversing the arm unless resistance is felt.” He adds that operators should follow the overall recommendations for radiation safety. Specifically, it is important to minimize patient exposure to cineangiography, which has a high radiation exposure rate.
Based on a review of limited literature—particularly the RIVAL (Radial Versus Femoral Access for Coronary Intervention) and RIFLE-STEACS (Radial Versus Femoral Randomized Investigation in ST-Elevation Acute Coronary Syndrome) trials—the SCAI expert panel established a consensus on the transition by operators and sites from mostly performing transfemoral primary PCI to transradial primary PCI. “We recommend that both the operator and the site perform at least 100 elective procedures using a radial-first approach—with a femoral crossover rate of 4% or less—before performing transradial primary PCI,” says Dr. Rao.
The consensus document also recommends that clinicians consider bailouts to either contralateral radial or femoral access if the time to obtain radial access exceeds 3 minutes. A bailout should also be considered if the time from introducer sheath placement in the radial artery to engaging the infarct-related artery with the guide catheter exceeds 10 minutes. The same is also true if the total time from radial artery introducer sheath placement to dilating the infarct lesion exceeds 20 minutes.
Unanswered Transradial Questions
“More information is needed on the interaction between radial access and pharmacotherapy,” Dr. Rao says. “Research shows that the radial approach reduces access site bleeding, but non-access site bleeding is still an issue. Whether an interaction or synergy exists between using certain pharmacologic agents and radial access needs to be explored.” Dr. Rao adds that many operators avoid using the radial approach in patients with abnormal Allen’s test or abnormal Barbeau test results, despite a dearth of data supporting the avoidance of these patients.
A better understanding of the best approaches to teaching transradial procedures is also necessary, says Dr. Rao. “This includes identifying the elements of a good training program and whether proctorship makes a difference. This is applicable to radial procedures as well as all new procedures that emerge in interventional cardiology. More evidence-based approaches are needed when teaching physicians how to perform surgical procedures. In the meantime, providers can turn to the SCAI consensus document for evidence-based best practices to enhance their use of transradial angiography.”
 TimH
TimH
{kind=link}
{kind=link}