
Following the recent FDA approval of new medications to reduce cardiovascular death and heart attack in patients with acute coronary syndromes (ACS) and developments in the literature, the American College of Cardiology (ACC) and American Heart Association (AHA) released a focused update to 2007 guidelines on the management of patients with unstable angina (UA)/NSTEMI. The update, published in Circulation, focuses on how antiplatelets and anticoagulants fit into management algorithms for ACS.
Key Updates to UA/NSTEMI Guidelines
An important change in the ACC/AHA guideline update is that ticagrelor is now considered a treatment option for UA/NSTEMI patients, joining clopidogrel and prasugrel. “We recommend that when aspirin is given with ticagrelor for maintenance therapy, a low dose of aspirin (81 mg) should be used after the initial loading dose,” says Jeffrey L. Anderson, MD, FACC, FAHA, co-author of the guidelines. “Research shows that a high dose of aspirin appears to reduce the benefits of ticagrelor.”
Aspirin remains a first-line therapy for managing patients with UA/NSTEMI. “When these patients arrive at the hospital, they should receive aspirin and an anticoagulant,” says Dr. Anderson. “Clinicians should then decide upon a second antiplatelet agent before angiography to define coronary anatomy. Clopidogrel, ticagrelor, or an intravenous glycoprotein IIb/IIIa agent are acceptable options. At or after coronary stenting, prasugrel becomes an additional option.” For patients receiving medical therapy only, the ACC/AHA guidelines recommend antiplatelet therapy with ticagrelor or clopidogrel, in addition to aspirin.
Several changes were made in the guideline update regarding patients with renal insufficiency. “It’s important to assure that these patients are well hydrated if they’re going to the cath lab and that they receive the minimal amount of contrast agent, which can cause renal toxicity,” Dr. Anderson explains. “While an invasive strategy among higher-risk patients with mild-to-moderate renal insufficiency appears to be more effective than a conservative approach, we still lack enough data to conclude that such a strategy is preferable in patients with advanced renal failure.”
Classifying Patients: Invasive Vs Conservative UA/NSTEMI Therapy
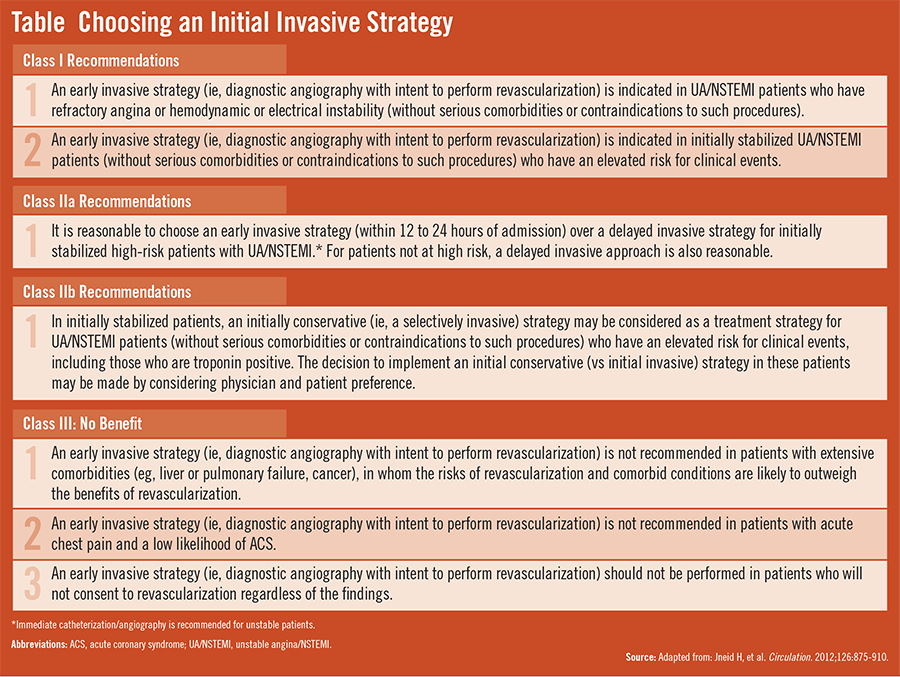
The ACC/AHA guidelines stress the need to stratify risk in patients with apparent UA/NSTEMI when choosing between invasive or conservative initial therapy. Dr. Anderson says that patients at low risk for adverse outcomes, particularly women, should not receive invasive therapy. “The more aggressive medical therapies may cause more bleeding, and the costs aren’t justified,” he adds. “Invasive therapy generally should be reserved for those with a definitive diagnosis of UA/NSTEMI and moderate- to high-risk features [Table].”
With an invasive management strategy, anticoagulants should be initiated, according to the guidelines (Figure). “Acceptable options are unfractionated heparin or low molecular-weight heparin (LMWH),” says Dr. Anderson. “For patients who will enter the cath lab within 12 hours, unfractionated heparin is a popular choice because of its rapid onset and offset. LMWH is often chosen when there is a longer delay to the cath lab. Bivalirudin is an increasingly popular option in the cath lab.”
“It’s important to stratify patients by risk as early as possible.”
During the pre-catheterization period, a second antiplatelet should be added, with the choices noted above. After PCI, an oral P2Y12 inhibitor should be given for 12 months, along with aspirin indefinitely. For patients who have undergone bypass surgery, aspirin is recommended as maintenance antiplatelet therapy.
With an initial conservative strategy, an anticoagulant also is recommended. Acceptable choices are unfractionated heparin, LMWH, or fondaparinux. “Because patients managed with a conservative strategy may be treated for several days with an anticoagulant, unfractionated heparin is not preferred,” says Dr. Anderson. “That’s because it’s associated with an increased risk of heparin-induced thrombocytopenia. Enoxaparin or fondaparinux are the preferred anticoagulants in this setting. Bivalirudin, which has not been tested in this setting, is not recommended.” Clopidogrel and ticagrelor are the antiplatelet agent choices, added to aspirin, and given for up to 1 year. If recurrent angina occurs or if a post-ACS stress test or advanced imaging test indicates high residual ischemic risk, coronary angiography should be performed.
Adopting Strategies for UA/NSTEMI Management
While it is encouraging that more effective strategies now exist for managing UA/NSTEMI patients, Dr. Anderson says clinicians must still be vigilant in evaluating bleeding risk, choosing therapies, and adjusting medication doses. “It’s important to stratify patients by risk as early as possible. Classifying patients as being a definite or likely candidate for certain treatments is paramount before aggressive therapies like anticoagulants and antiplatelets should be initiated. Clinicians should refer to the AHA/ACC guideline update to enhance their ability to provide patients with the best possible care.”
 admin
admin
{kind=link}
{kind=link}