

It has been estimated that 5,000 to 10,000 aortic dissections occur in patients each year in the United States, and nearly one-third of these individuals will die before hospital discharge. Despite recent advances in diagnostic tools and surgery, the tearing of the aorta can be challenging for even the most experienced cardiovascular specialists to diagnose. In 2010, the American Heart Association and American College of Cardiology released clinical guidelines—developed in collaboration with 10 professional societies—for the diagnosis and management of thoracic aortic disease, emphasizing high-risk clinical features that indicate the presence of acute aortic dissection (AAD). Validation of these risk markers had yet to occur until the results of a study by the University of Michigan Cardiovascular Center (UMCC) published in 2011 in Circulation, which suggested patients with certain characteristics were likely to be suffering from an aortic dissection.
“Over the past 20 years, much progress has been made in various facets of thoracic aortic disease,” says Kim A. Eagle, MD, co-author of both the guidelines for thoracic aortic disease and the aforementioned UMCC study. “This includes a better understanding of the natural history of thoracic aortic disease and the potential genetic factors that may underlie some of the aortic problems of the thorax. There has also been an evolution of modern imaging techniques for more reliable and speedy diagnoses and follow-up. Furthermore, new strategies for both medical and interventional therapy have emerged.” (see also, Strategies for Managing Thoracic Aortic Disease With Surgery).
When compared with coronary heart disease, hypertension, or heart failure, thoracic aortic diseases are rarer, and therefore, probably encountered by practitioners less frequently. “As a result,” adds Dr. Eagle, “physicians may not necessarily have as much experience with these problems and may feel less comfortable knowing the most appropriate strategies by which to diagnose and treat these individuals. In addition to the high mortality rate associated with thoracic aortic disease, concern over patient management has been a major reason why the various professional societies felt it was important to put together guidelines to assist physicians. We now have data available that help put into context what is currently known about the optimal management of these patients.”
Strong Focus on Acute Aortic Dissection
According to Dr. Eagle, the guidelines provide a large section on AAD, including the aortic dissection risk score. “This tool provides a way for providers— especially acute care specialists and those working in EDs—to increase the likelihood that they will identify AAD early and provide faster, life-saving therapy.” Using a simple, bedside screening tool, the AAD risk score was shown in the UMCC study to help physicians identify the signs and symptoms of AAD in most cases (see also, Managing Thoracic Aortic Disease).
“It was important for clinicians to create a tool that can help identify AAD in a more reliable way,” says Dr. Eagle. “We established a set of clinical variables that should be ascertained and considered when evaluating patients with acute abdominal or thoracic discomfort [Table 1].” The guidelines recommend considering AAD in patients who have had a recent aortic manipulation; chest, back, or abdominal pain that has abrupt onset, very severe intensity, or ripping or tearing quality; and evidence of a perfusion deficit in any of the arteries. They also recommend considering AAD in the presence of a new murmur or aortic valve insufficiency or in the presence of very low blood pressure or shock. Dr. Eagle noted that this information can typically be ascertained in about a minute.
In the UMCC study, about 96% of patients with aortic dissection had at least one of the 12 markers now identified in the guidelines. Roughly 86% had two or more markers. “By taking a careful history of these predisposing conditions and the pain that typically accompanies these patients, the risk of dissection can be categorized as high enough to warrant further investigation,” says Dr. Eagle.
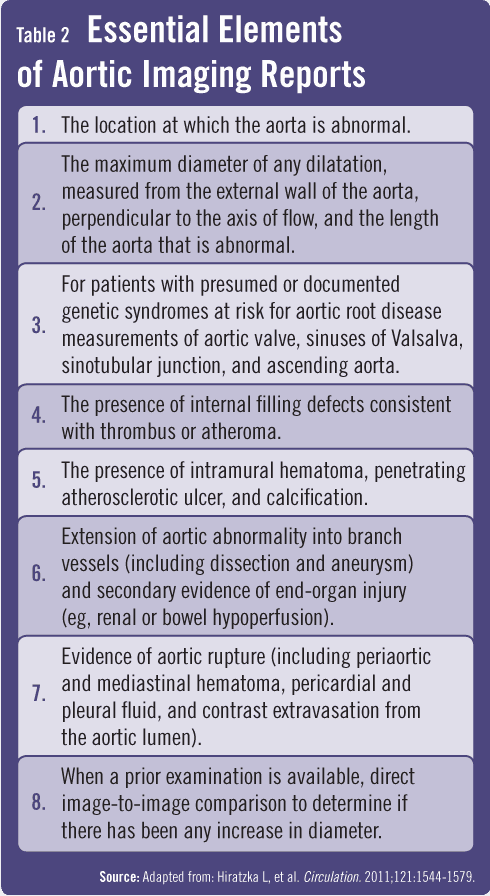
Further investigation in the ED to identify dissection should include CT scans or transesophageal echocardiography (Table 2). Dr. Eagle adds that “if the aorta is torn but not dilated, an x-ray will be normal because patients with AAD don’t always have a widened aortic shadow on x-ray.” He also warns that pain begins suddenly in patients with AAD, but that pain often subsides, giving a false sense of reassurance.
Raising Awareness of Acute Aortic Dissection
The Thoracic Aortic Disease Coalition represents a group of national societies, academic leaders, and institutions. It aims to increase awareness about aortic disease among the lay audience as well as clinicians. Dr. Eagle says “it’s important that physicians, nurses, and the public better understand thoracic aortic disease because it can be disastrous when it strikes.”
 Janine Anthes
Janine Anthes
![[Table 1]](https://www.physiciansweekly.com/wp-content/uploads/2012/05/Eagle-Table-1.png){kind=link}
{kind=link}