

Each year, about 1.2 million Americans survive an acute coronary syndrome (ACS) event, many of whom have clinically significant and persistent depression. “Post- ACS depression has been associated with higher risk of ACS recurrence and a doubling of increased risk of all-cause mortality,” explains Karina W. Davidson, PhD. “Persistent depression after an ACS event correlates with an even higher morbidity and mortality risk. Considering its burden on the healthcare system, efforts to reduce persistent post- ACS depression are important.”
Despite knowledge of these associations, routine management of depression after ACS events remains poor. Historically, clinicians have been inefficient in screening for depression and lack effective approaches to treating it. Further compounding the problem are the weak effects often linked to depression treatments and limited options if initial therapies and efforts fail. For patients who have had an ACS event, psychotherapy and/or psychotropic medications are oftentimes not integrated into care.
The CODIACS Vanguard Trial
At ACC.13, Dr. Davidson and colleagues presented results from the Comparison of Depression Interventions after Acute Coronary Syndrome (CODIACS) Vanguard trial. It was designed to determine the feasibility, efficacy, and costs of a centralized, stepped, patient preference–based depression care system for patients after experiencing an ACS event. The study, which was also published in JAMA Internal Medicine, involved 150 patients who had depression scores of 10 or higher (out of 60) on the Beck Depression Inventory (BDI) scale 2 to 6 months after an ACS event.
“CODIACS Vanguard was designed to provide depression treatment several months after an ACS,” explains Dr. Davidson, who was lead author of the trial. “This is when most transient depressive reactions to ACS have spontaneously remitted, but the prognostic risk of ongoing depression symptoms is still high. The treatment strategy in CODIACS Vanguard incorporated patient preferences and adjusted treatment in a stepped manner as symptoms required.”
Patients in the study were randomized to 6 months of centralized depression care, which factored in patient preferences for problem-solving treatment (given via telephone or the internet), pharmacotherapy, both, or neither. The intervention was stepped every 6 to 8 weeks for the active treatment group if minimum improvement was not seen on the Patient Health Questionnaire 9. The usual care group was permitted to get treated for depression by their primary care physician, cardiologist, or another healthcare provider.
Depression Outcomes Among ACS Patients
According to results, the intervention tested in the CODIACS Vanguard trial led to significant decreases in depressive symptoms among ACS patients when compared with the usual care group (Table). BDI scale scores decreased by 3.5 points more for those receiving stepped care with problem-solving treatment and/or pharmacotherapy than those in the usual care group. “We also observed improvements in remission of depression for the active treatment group,” adds Dr. Davidson. Remission of depression—defined as a BDI score of less than 10 when measured at 6 months— occurred in 47.1% of active treatment patients, compared with a 27.6% rate for usual care patients.
In subgroup analyses, BDI scores decreased more in women than in men in the active treatment group (-6.4 vs -1.6, respectively). Patients with diabetes experienced greater decreases in BDI scores than those without the disease in the active treatment group (-6.2 vs -0.9). No other subgroup differences were found, including a comparison of ACS patients with different levels of depression.
Healthcare Costs Among Patients With ACS
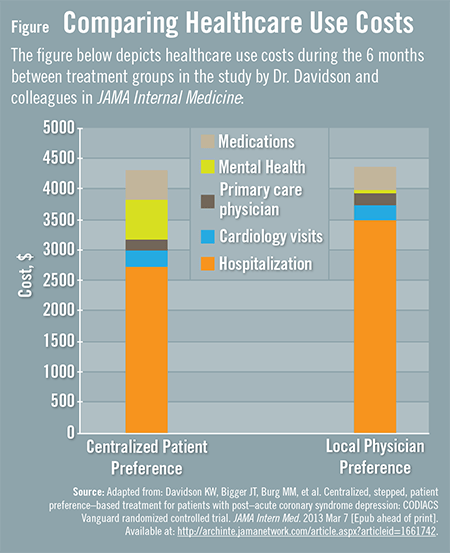
The CODIACS Vanguard trial also found that the estimated mental healthcare costs were higher for active treatment than for usual care, but the overall healthcare costs were not significantly different between groups. “For the active treatment group, mental health costs were $687 higher than for the usual care group, but average hospital costs were $1,010 lower,” explains Dr. Davidson (Figure). “This was mainly due to fewer hospitalizations in the active arm.” As a result of this offset, total healthcare costs for the active treatment group were not higher than those receiving usual care.
Acute Coronary Syndrome: Looking Ahead
Findings from the CODIACS Vanguard trial provide a basis for future studies to determine whether treating depression can decrease the risk of death and reduce recurrence of cardiac events in patients with an ACS event, according to Dr. Davidson. “Further study is required, but we now have new signals of a substantial and potentially cost-neutral depression treatment benefit from this and other randomized control trials. This information can be used to develop a definitive ACS depression trial. A large phase III trial would further enhance treatment guidelines for patients who have ACS events. Such data may enable us to eventually determine whether or not treating depression in patients with ACS truly lowers mortality and recurrence rates.”
 admin
admin
{kind=link}
{kind=link}