

The steady increase in use of prescription opioids in the United States over the past decade has been a key contributor to the sky-rocketing incidence of abuse of these medications. The number of opioid prescriptions written for pain has risen from about 76 million in 1991 to approximately 219 million in 2011. In conjunction with this rising prescription rate has been an increase in opioid-related overdoses and hospitalizations. “With their increasing availability, prescription opioids have become the most abused class of drug in the U.S.,” says Robert N. Jamison, PhD. Research shows that more deaths are related to opioid abuse than cocaine and heroin combined.
The OCC
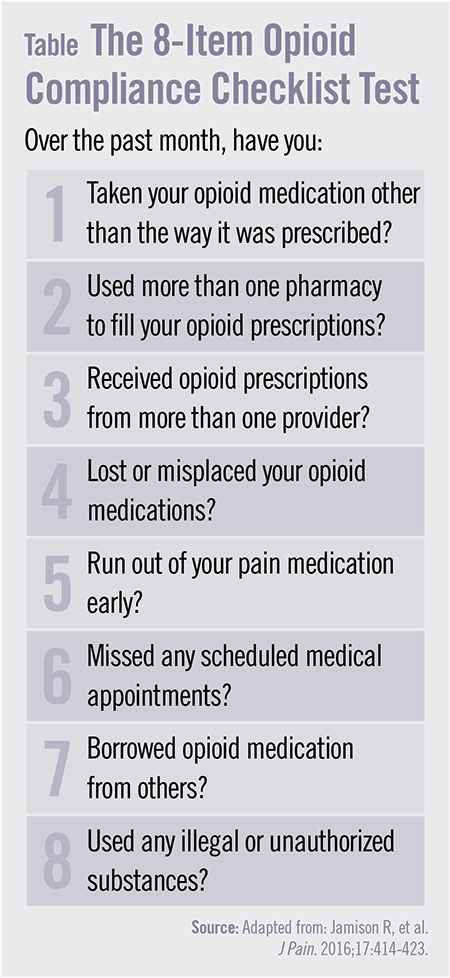
Studies indicate that most clinicians are not adequately prepared to properly diagnose, treat, and monitor patients with chronic pain who are prescribed opioids. To address this issue, researchers have developed the Opioid Compliance Checklist (OCC), a brief, self-report measure to help document opioid compliance for use by prescribing practitioners. “It was designed to reflect components of an opioid therapy agreement that would outline patients’ responsibilities and clinic policies in prescribing opioids for chronic pain,” adds Dr. Jamison.
In a previous study, the original items of the OCC were administered to 157 chronic non-cancer pain patients who were taking long-term opioids and being cared for at pain specialty centers. Participants were followed for 1 year to evaluate evidence of non-compliance and aberrant medication-related behavior. Nearly 45% of patients had a positive Drug Misuse Index score based on either positive urine toxicology results, self-report measures, and/or physician-rated aberrant drug-related behavior. However, the study concluded that there was a need to validate the OCC in chronic pain patients in the primary care setting to determine the most clinically useful items among patients in a non-specialty center.
New Data
For a study published in the Journal of Pain, Dr. Jamison sought to determine the effectiveness of an eight-item OCC (Table) for monitoring opioid compliance with a new sample of patients from multiple primary care centers who were prescribed long-term opioids for pain. The analysis involved 177 individuals from eight primary care institutions, and all participants completed pre- and post-study measures as well as the OCC once a month for 6 months. Patients were then classified on the Drug Misuse Index based on results of urine toxicology screens, physician misuse behavior ratings, and self-report questionnaire results.
According to the results, patients treated in primary care reported fewer incidences of opioid misuse when compared with those from pain specialty centers in the original study. “Patients who answered ‘yes’ to any of the eight OCC questions were at risk for current or future opioid misuse,” says Dr. Jamison. By the end of the study, patients who regularly took the OCC had greater compliance with their opioid medication.
A Helpful Tool
Results of the study suggest that the OCC appears to be a reliable and valid screening tool to help detect current and future aberrant drug-related behavior and non-adherence among chronic pain patients in primary care, according to Dr. Jamison. “Repeating the OCC among patients taking opioids for chronic pain can increase the chance of identifying those misusing or likely to misuse opioids,” he says. “Periodically asking the questions in the OCC may remind patients about being responsible about their opioid use.”
The study group noted that differences were observed between patients seen in a specialty pain center and those treated within primary care. Overall, patients receiving pain care from primary care centers had a lower incidence of opioid misuse and tended to have fewer “yes” responses on the OCC when compared with pain patients seen at specialty pain centers.
Potential Benefits
Dr. Jamison says the OCC is a tool that can be used to alert physicians about ongoing risk behaviors so that they can intervene to avert future problems with opioids. “This tool can help us document patient responses to the OCC, which could be useful when deciding if patients need closer or more frequent monitoring or if they should discontinue therapy,” he says. “The OCC is relatively quick and easy to administer—taking about 2 minutes to complete on average—within busy clinics after a formal risk assessment has been obtained from patients who are prescribed opioids.”
Although patients could easily deceive physicians with their self-reported answers on the OCC if they so desired, participants tended to be truthful in their responses to the test. “It’s critical for providers to consider the OCC results in the context of information from other sources,” says Dr. Jamison. “This includes the patient’s history and physical exam, the clinical interview, discussions with family members, laboratory findings, and a review of medical records. When used appropriately, the OCC offers clinicians a way to monitor misuse behaviors and then, when appropriate, develop treatment strategies to minimize continued misuse.”
 PWeekly
PWeekly
{kind=link}