

Attending rounds has been a long-standing practice for internal medicine physicians, residents, and medical students to direct patient care, communicate with patients and families, and advance their medical education. The model of having senior physicians, trainees, and patients interact has existed for decades, but the features of these rounds have evolved dramatically in more recent years, explains Chad Stickrath, MD. “The format has shifted away from being conducted mostly at the bedside to taking place more frequently in conference rooms and hallways.”
The Accreditation Council for Graduate Medical Education (ACGME) program requires that patient-based teaching include direct interaction between residents and attending physicians, bedside teaching, discussion of pathophysiology, and the use of current evidence in diagnostic and therapeutic decisions. The ACGME does not, however, provide additional specific guidelines on how to accomplish these requirements. The structure and content of contemporary attending rounds has not been well described in studies. “Some educators have expressed concerns about how patient communication and physical examination skills are being deemphasized,” adds Dr. Stickrath.
Are Patient Rounds Meeting Goals?
In a study published in JAMA Internal Medicine, Dr. Stickrath and colleagues sought to determine if current methods of patient rounds are meeting patient care and educational goals. The cross-sectional observational analysis was conducted at four teaching hospitals, involving 56 attending physicians and 279 trainees who treated 807 general medicine inpatients. The study group performed detailed observations of 90 rounds over a course of nearly 2 years.
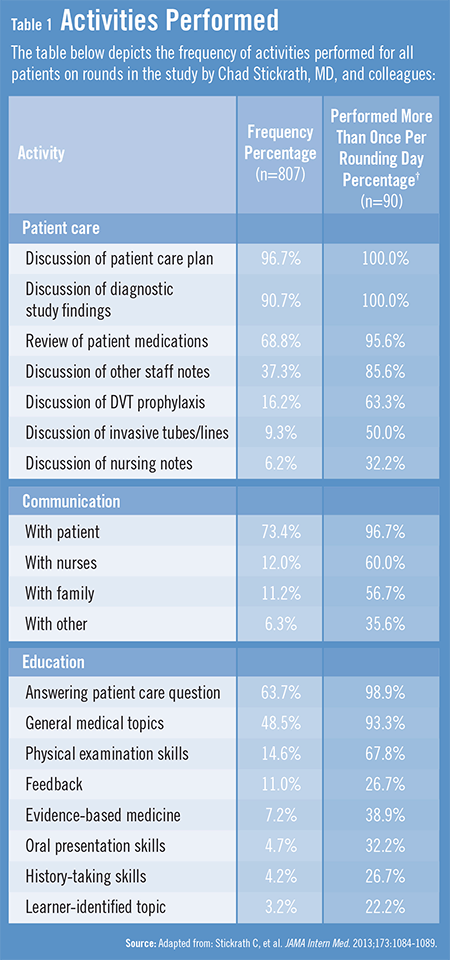
According to results, most rounds consisted of an attending physician and several resident and student trainees, speaking with a median of nine patients during the course of about 2 hours. On rounds, general medical teams most frequently discussed patient care plans, reviewed diagnostic studies, communicated with patients, and discussed medication lists (Table 1). Teams rarely communicated with nurses or taught physical examination skills or evidence-based medicine topics.
“Much time was dedicated to discussing patient care plans and drug lists in our analysis,” Dr. Stickrath says. “Communication with patients was frequent, especially when rounds were conducted at the bedside. However, other important care issues, such as DVT prophylaxis and the presence of invasive tubes and lines, were infrequently discussed. In addition, interprofessional communication on rounds appeared to be lacking. The need for effective communication between physicians and other care providers has never been more important. Poor interprofessional communication can be detrimental to care, but interventions to improve this communication can improve processes and outcomes.”
Time Limited at the Bedside
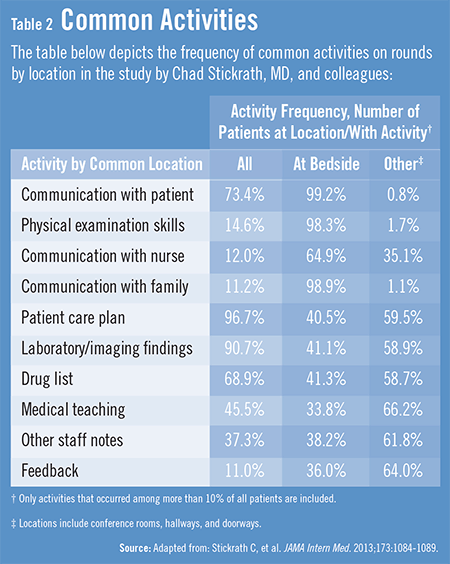
The study by Dr. Stickrath and colleagues also found that most activities were more often performed away from the bedside, such as general medical topic teaching, feedback, and discussion of patient care plans, diagnostic studies, and patient medication lists (Table 2). However, some activities were performed nearly exclusively at the bedside. These included most communication activities and the teaching of physical examination skills. “We also found that teaching about learner-identified topics on rounds was rare,” says Dr. Stickrath. “Using learner-
centered teaching models during attending rounds may improve the educational environment.”
Prior to duty-hour restrictions that were mandated in 2003, attending rounds typically lasted about 90 to 100 minutes. After implementing those restrictions, studies suggest that rounds last longer, meaning there is less time for formal training. “In our study, rounds lasted an average of 122 minutes, which represented a significant amount—about 15%—of total training time for a given week,” explains Dr. Stickrath. “Our observed increase in the duration of attending rounds suggests that teaching must be efficient and effective.”
The Bigger Picture of Physician Education
The emphasis on patient safety and preventing medical complications continues to grow, and Dr. Stickrath says that attending rounds is an important component to achieving these goals. “Attending rounds give us a natural opportunity to discuss important issues with trainees and a chance to address preventable medical complications,” he says. “The training of attending physicians in their role appears to affect how they communicate with interprofessional team members and provide feedback to trainees. Attending physicians need to be confident in their ability to teach.”
Although the study may not be representative of attending rounds on a wider scale, the findings have important implications. “Trainees have less time to spend on providing patient care and engaging in medical education, but attending rounds present an increasingly precious opportunity to do both,” Dr. Stickrath says. “We must continue to assess the effect that certain characteristics and teaching models of rounds have in order to optimize patient care and physician education in the future.”
 admin
admin
{kind=link}
{kind=link}