

National estimates indicate that asthma and COPD are the most common diagnoses for patients with breathlessness and airway obstruction, each affecting greater than 5% of the United States population. These conditions often share similar characteristics, most notably chronic airway inflammation and hyper-reactivity. Recently, the Global Initiative for Chronic Obstructive Lung Disease guidelines for diagnosing, managing, and preventing COPD recognized asthma-COPD overlap syndrome (ACOS) as a separate entity. ACOS occurs in patients with fixed airway obstruction that defines COPD who also have symptoms that are more typical of asthma, such as wheezing. The prevalence and comorbidities associated with this syndrome have not been well defined in clinical research.
Surveying the Scene
For a study published in the Annals of the American Thoracic Society, Charlie Strange, MD, and colleagues used data from the 2012 Behavioral Risk Factor Surveillance System (BRFSS). “In each state, 10,000 people were interviewed, allowing for a cross sectional analysis of the entire population,” says Dr. Strange. “Many people who don’t access the healthcare system could be interviewed. For the first time, in 2012, 11 states added a module to the traditional survey that asked questions about COPD. This allowed us to capture symptomatic patients with a dual diagnosis, as current asthma was already being queried.”
Among respondents to the BRFSS who were older than 35, the study team compared self-reported demographics, smoking status, comorbidities, and hospitalizations or emergency department (ED) visits. Patients with ACOS were then compared with those who had COPD, asthma, or neither of these conditions.
Examining Results
Dr. Strange and colleagues found that the prevalence of ACOS (3.2%) was less than the prevalence of COPD alone (6.0%) or asthma alone (5.6%). The prevalence rates of ACOS and COPD both increased with age, particularly with COPD after the age of 65, whereas the prevalence of asthma alone decreased with age. On average, participants with ACOS were younger than those with COPD and older than those with asthma. “It has been known for years that asthma is more prevalent in younger people and that COPD increases with age,” says Dr. Strange. “However, it’s a new finding that ACOS prevalence continues to increase up to age 85.”
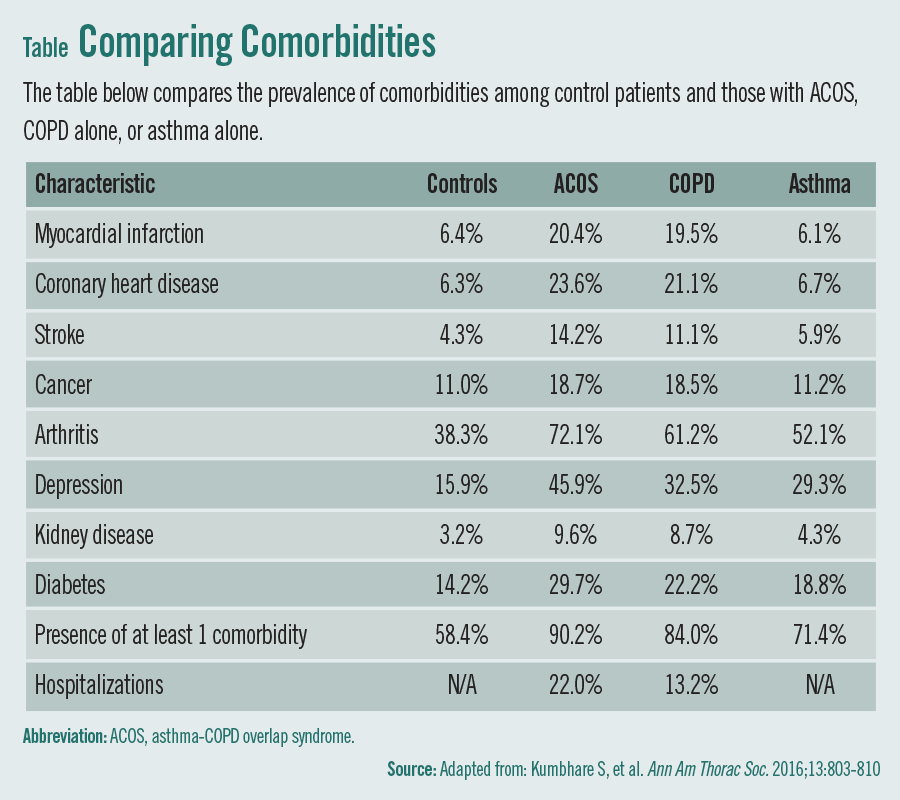
Patients with ACOS were more likely to have other comorbidities than those with COPD. Participants with COPD had a higher prevalence of comorbidities than those with asthma and the control group that was analyzed in the study (Table). The research team noted that patients with ACOS generally had higher BMIs, lower income levels, and less education than other groups of study participants..
“Overall, the ACOS group was more likely to have at least one comorbidity and had more hospitalizations or ED visits than the COPD group,” Dr. Strange says. “This group also exercised less and tended to experience more disability. Additionally, patients with ACOS were more likely to have coronary artery disease, depression, and diabetes. These are highly prevalent diseases that aren’t obviously related to lung disease. It’s possible that these patients are more likely to have poor access to healthcare, which in turn could mean that they have a lower likelihood of receiving a specific diagnosis. It’s also likely that treating patients with ACOS costs the healthcare system much more than caring for those with asthma or COPD alone.”
Addressing Implications
By recognizing the importance of patients with ACOS receiving an independent diagnosis, Dr. Strange says more studies can be conducted to determine which medications are best suited for this specific population. “These patients typically are not included in clinical trials because many who have a COPD diagnosis or smoke are excluded from asthma trials,” he explains. “Also, those with an asthma diagnosis are often excluded from COPD trials.”
Related Articles
- Fruit, Vegetable Consumption Linked to Lower Risk of COPD
- Serum Periostin IDs Comorbid Chronic Rhinosinusitis in Asthma
- Asthma Drugs Could Prevent Deadly Form of Pneumonia
- Understanding COPD-Overlap Syndromes
According to Dr. Strange, patients with ACOS are unique and use many healthcare resources. “It’s critically important that clinicians learn more about this patient group,” he says. “This requires more studies focusing on factors like the efficacy of inhaled steroids, strategies for preventing hospitalizations, and the role of BMI on patient outcomes.”
In the meantime, Dr. Strange says clinicians should closely examine the comorbidities of patients who appear to have ACOS. “Screen for depression, assess A1C levels, discuss cardiovascular risk factors and assure they’re seeing a cardiologist, and order a lipid panel to check cholesterol levels, for example, as opposed to focusing only on their lungs,” he says. “In general, clinicians who treat COPD and asthma need to be more comprehensive in addressing the comorbidities that come with these diseases.”
 PhysWeekly
PhysWeekly
{kind=link}