
According to recent estimates, about half of all cancers and 70% of all cancer deaths occur in people aged 65 and older. Gastrointestinal cancers, especially colorectal cancer (CRC), are among the most common to afflict the elderly, with peak incidences occurring when they reach their 60s and 70s. However, while the population continues to age, clinical research trials often exclude these individuals. This raises a concern that data from these investigations may not accurately reflect the true morbidity and mortality in the elderly.
“The surgical community needs to recognize the aging shift that’s occurring in the United States and prepare accordingly,” says Mehraneh D. Jafari, MD. Efforts have increased to screen more patients for CRC, but it remains the third-leading type of cancer and second-leading cause of cancer-related deaths. Surgical resection is a curative modality for CRC, but studies suggest that most patients seek treatment after they have reached their 70s.
Examining Trends
“Few national studies have assessed the effects of age on morbidity and mortality in CRC and analyze the latest trends in surgical resection in the elderly,” says Dr. Jafari. In JAMA Surgery, Dr. Jafari teamed with Michael J. Stamos, MD, and colleagues to publish a study that sought to address this knowledge gap. The study was unique in that it assessed trends among CRC patients undergoing surgical resection while also examining small incremental age increases and the effects on overall morbidity and mortality over the past decade.
For the analysis, operative outcomes after CRC surgery were reviewed using data from the Nationwide Inpatient Sample. Patients were stratified within age groups, and postoperative complications and yearly trends were analyzed to compare in-hospital mortality and morbidity between groups. “Among the more than one million patients sampled,” says Dr. Stamos, “about two-thirds of CRC operations were performed on those aged 65 and older, whereas almost one-fourth (22.6%) were on patients aged 80 and older.”
Morbidity & Mortality
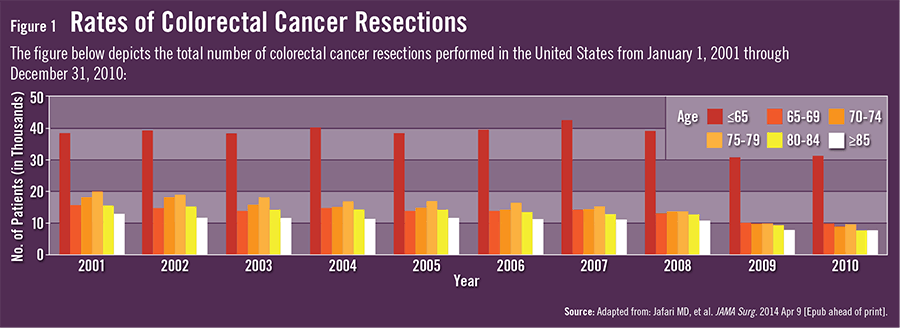
During the 10-year study period, the total number of CRC resections decreased by an average of 5.1% annually for the entire population and 7.0% per year for the aging population (Figure 1). Patients aged 80 and older were 1.7 times more likely to be urgently admitted to the hospital than those younger than 65. “With the issuing of national CRC screening recommendations, it was assumed that fewer patients would need to undergo urgent admissions,” says Dr. Stamos. “However, our data indicated that CRC screening efforts may be lacking for patients aged 80 and older.”
Patients aged 65 and younger accounted for 46.0% of the laparoscopic operations performed in the elective setting, compared with 14.1% for patients aged 80 and older. Those aged 80 and older also had hospital charges that were nearly $9,500 higher and spent 2.5 more days in the hospital, on average, when compared with patients younger than 65. Many complication rates were not statistically different among the age groups, but rates of acute renal failure, cardiac complications, respiratory failure, urinary tract infections, and pneumonia rose as age increased. When compared with patients aged 45 to 64, higher risk-adjusted in-hospital mortality and morbidity rates were observed in patients with advancing age.
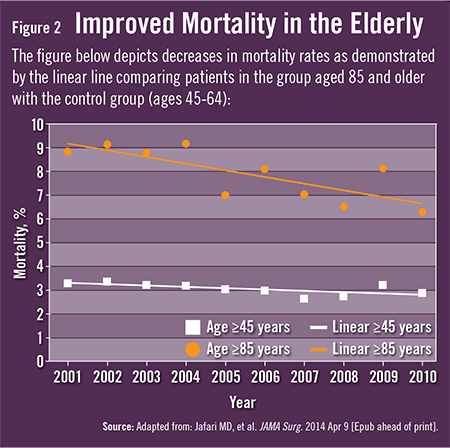
The study also showed that mortality rates decreased by an average of 6.6% over 10 years, with the most considerable decreases seen in patients aged 85 and older (Figure 2). “These decreases in mortality can probably be attributed to improved surgical techniques as well as a better understanding of the physiologic demands of these patients,” says Dr. Stamos.
Vigilance Required
Dr. Jafari says that despite the trend toward higher mortality and morbidity as CRC patients get older, there has been a marked improvement in surgical outcomes in the elderly. “The data are encouraging, but it’s still important to consider other factors during preoperative decision making,” she says. Postoperative complications can lead to higher costs, longer lengths of stay, and decreased quality of life, especially in the elderly, because they often have a lower functional reserve. “Elderly CRC patients will need vigilant postoperative care,” adds Dr. Stamos. “We should also consider each person’s unique needs during preoperative counseling and postoperative planning.”
Since most CRC resections are performed on patients aged 65 and older, measures should be implemented to improve outcomes in all settings. Many of these patients will require nursing facilities for rehabilitation after surgery. “Our quantifiable data provide clinicians with tools to help counsel patients,” says Dr. Jafari. “They serve as a reminder to reevaluate our current care patterns and reinforce the need for future analyses to account for the changing population landscape.”


{kind=link}
{kind=link}