
The geriatric population in the United States is growing at a faster rate than the total population, and there will be an increasing need for healthcare among this patient group. “The aging population represents an unprecedented and overwhelming challenge to the healthcare system as a whole and to EDs specifically,” says Mark S. Rosenberg, DO, MBA, FACEP. Studies show that geriatric patients have 20% longer ED lengths of stay and use 50% more laboratory and imaging services than younger patients. Geriatric ED patients are also significantly more likely to require social services.
It has been suggested that contemporary emergency medicine management models may be inadequate to care for the geriatric patient population. Published studies show that ED physicians often feel that they lack the proper training to manage geriatrics. “It’s challenging for ED physicians to manage older adults because they often have other medical comorbidities, take multiple medications, and present with complex physiologic changes,” Dr. Rosenberg says. “Programs specifically designed to address these concerns may substantially improve care. As the initial site of care for many health events, EDs have the opportunity to set the stage for subsequent care.”
Geriatric EDs
To enhance geriatric patient care in the emergency medicine setting, institutions throughout the U.S. have developed geriatric EDs, which are EDs dedicated to caring for older adults. The first such institutions appeared in the U.S. in 2008, but geriatric EDs have become increasingly common since that time. In response to the proliferation of geriatric EDs, the American College of Emergency Physicians (ACEP), the American Geriatrics Society, the Emergency Nurses Association, and the Society for Academic Emergency Medicine issued a comprehensive set of geriatric ED guidelines that took 2 years to complete. “The overriding goal of the guidelines is to provide a standardized template for how these facilities should be set up and how care should be delivered,” says Dr. Rosenberg, who was chair of ACEP’s geriatric ED guidelines task force.
A Comprehensive Resource
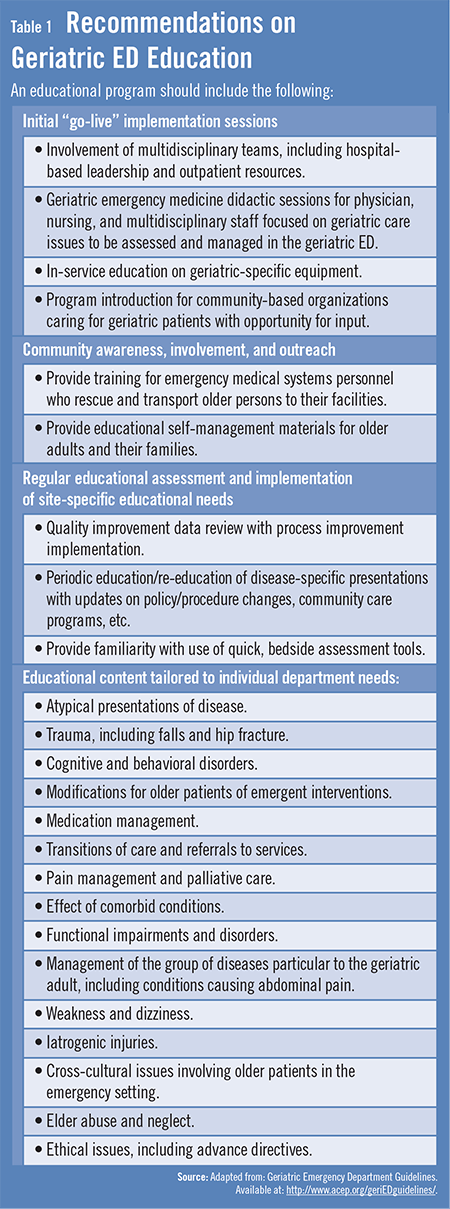
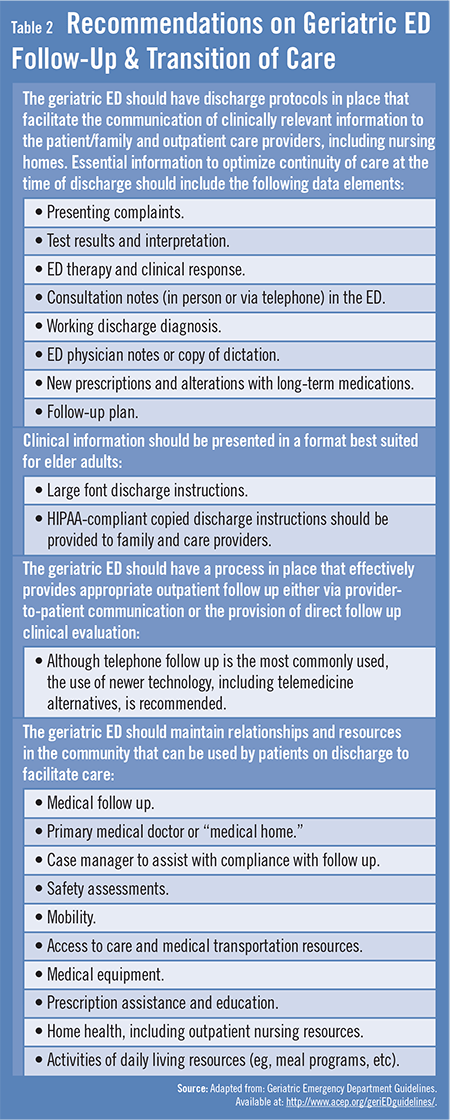
The geriatric ED guidelines cover many important topics to meet the special needs of these patients in the emergency setting. The document provides recommendations on geriatric ED education (Table 1) and follow-up and transitions of care (Table 2). It also offers information on staffing, quality improvement, equipment and supplies, and policies, procedures, and protocols. More specific information is provided on the use of urinary catheters, medication management, fall assessment, delirium and dementia, and palliative care.
“When implemented collectively, geriatric EDs can expect to see improvements in patient care, customer service, and staff satisfaction,” Dr. Rosenberg says. “By addressing the needs of this challenging patient population, we can be more effective at allocating healthcare resources.” Geriatric EDs can also help optimize admissions and readmission rates while simultaneously decreasing complication rates and the consequences of increased lengths of stay.
Important Benefits
According to the guidelines, an important goal of the geriatric ED is to recognize patients who will benefit from inpatient care and to implement outpatient care for those who do not require inpatient resources. The guidelines note that acute inpatient events are often accompanied by functional decline, increased dependency, and increased morbidity. “Geriatric EDs will need to use hospital, ED, and inpatient and outpatient resources to implement this approach effectively,” Dr. Rosenberg says. “Nurse practitioners, nurses, social workers, physician assistants, and physicians will be needed to coordinate care in EDs, inpatient units, and during the immediate discharge period.” Effective and expedient outpatient arrangements must also be made available to geriatric patients.
Dr. Rosenberg says that costs associated with establishing geriatric EDs are not necessarily exorbitant. “On average, it can cost as little as $1,500 per room to renovate an existing ED room and turn it into a geriatric ED room,” he says. “From a personnel standpoint, the staffing resources that are needed for converting to a geriatric ED already exist within the hospital. It just requires reallocating staff to accommodate the care of older patients in the ED. Overall, the benefits of geriatric EDs are multiple and clear. By standardizing and structuring these facilities appropriately, we can make geriatric EDs a significant marketing tool for hospitals.”
Significant Implications
Programs similar to geriatric EDs have been designed for other age groups and for specific diseases, such as heart attack, stroke, and trauma. These programs have improved care in individual EDs and throughout the healthcare system, resulting in more cost-effective and efficient care while also improving patient outcomes. “The concept of geriatric EDs takes a similar approach,” says Dr. Rosenberg. “By focusing our attention and resources on the most common needs of geriatric ED patients, we can further optimize care for this vulnerable patient population.”
 TimH
TimH
{kind=link}
{kind=link}