

In the December 6, 2011 Journal of the American College of Cardiology, the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) published guidelines on the management of patients undergoing CABG, one of the most common operations performed in the United States. These guidelines were released at the same time that the ACCF and AHA published recommendations for PCI. According to L. David Hillis, MD, FACP, chair of the ACCF/AHA guidelines committee for CABG, the landscape regarding when surgeons should perform CABG or PCI has been continually changing, particularly in the past 5 to 10 years. “Several recent investigations have shown that PCI and CABG have comparable outcomes when used in patients with certain coronary arterial anatomic features,” he says. “The last guidelines were published in 2004, but clinical trials have continued to improve our understanding of how to optimize the management of patients with coronary artery disease (CAD).”
A Collaborative Approach to Determine Revascularization
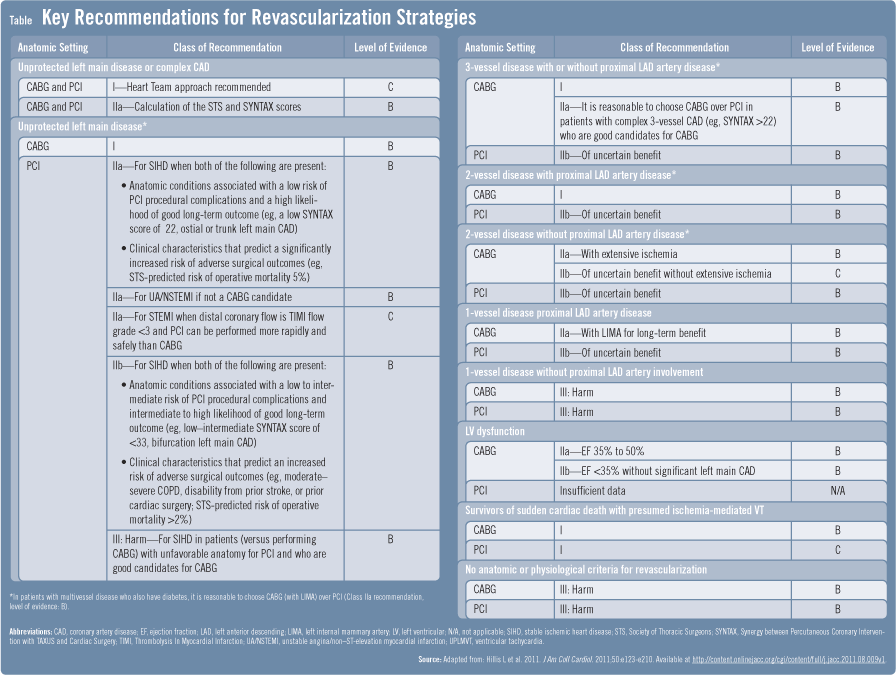
Through a collaboration of two writing committees, the ACCF/AHA guideline update contains the most extensive examination of CABG and PCI use for coronary revascularization. “While one committee was re-writing the CABG guidelines, a separate committee was revising the PCI guidelines,” explains Dr. Hillis. “Our goal was then to develop a consensus between cardiologists and surgeons over patient selection for these two procedures. Busy practitioners have historically been challenged when deciding on which patients should undergo revascularization rather than being treated medically, and whether revascularization should be accomplished with CABG or PCI.” Dr. Hillis says a section of the guidelines has been established to address questions that clinicians may have when deciding on using PCI or CABG (Table). “With the debate of PCI versus CABG heating up over the past decade, this information is likely to be of great interest to practicing physicians.”
“Clinical trials have continued to improve our understanding of how to optimize the management of patients with coronary artery disease.”
Decisions, Decisions…PCI or CABG?
Improvements in PCI technology have increased utilization of the procedure. PCI is now considered an acceptable substitute for CABG regardless of the severity of CAD, as long as patients’ anatomy is deemed suitable for PCI. “For example, 10 or 20 years ago, patients with left main CAD would have received CABG,” explains Dr. Hillis. “Factoring in the new data that have emerged, some of these patients are now candidates for PCI, particularly those with low risk of PCI-related complications and increased risk of adverse surgical outcomes. This will depend on information collected from coronary angiogram data as well as the patient’s age, comorbidities, and other factors.” Dr. Hillis notes that CABG, however, is still considered superior to medical therapy and PCI for many patients with three-vessel disease.
A Heart Team Approach
The ACCF/AHA guidelines strongly emphasize using a “heart team” approach, which will require a fundamentally different approach to how patients are managed. “In ‘real world’ settings, the decision on whether to perform PCI or CABG can vary significantly from patient to patient,” Dr. Hillis says. “With a heart team approach, interventional cardiologists and cardiac surgeons work together to review the patient’s condition and the pros and cons of each treatment option. They then present their findings and opinions to the patient so that an informed, collaborative decision can be made.”
Antiplatelet Therapy for CAD
The use of preoperative and postoperative antiplatelet therapy is also addressed in the 2011 ACCF/AHA guidelines. “Since 2004, more antiplatelet drugs have become available, further improving inhibition of platelet aggregation,” says Dr. Hillis. Among the currently available alternatives to aspirin are clopidogrel, glycoprotein IIb/IIIa inhibitors, and other agents. The guidelines recommend that aspirin be administered preoperatively to all CABG patients. Patients receiving elective CABG are advised to discontinue clopidogrel and ticagrelor for at least 5 days before the operation. Those undergoing urgent CABG should be taken off these agents for at least 24 hours before surgery, if possible. Administering aspirin within 6 hours postoperatively and continuing it indefinitely is also recommended. Patients who are allergic to aspirin are advised to take clopidogrel as a reasonable alternative.
Coronary Artery Disease: What’s On the Horizon
With continued improvements expected to occur in PCI and medical therapy, it is anticipated that CABG will increasingly be reserved for patients with extensive CAD. “CABG research will likely focus on improving results in high-risk patients and making the procedure a less invasive option for elective revascularization,” Dr. Hillis says. He adds that there are other promising treatment strategies on the horizon for patients with CAD, including the use of robotics and anastomotic connectors, intraoperative imaging, hybrid procedures that combine PCI and CABG, and protein and gene therapy. “More evidence is still needed on the selection of PCI or CABG in patients with CAD as well as these investigational treatment modalities,” adds Dr. Hillis. “The hope is that clinical studies will enhance our understanding of the best ways to optimize outcomes in these individuals.”
 Janine Anthes
Janine Anthes
{kind=link}