
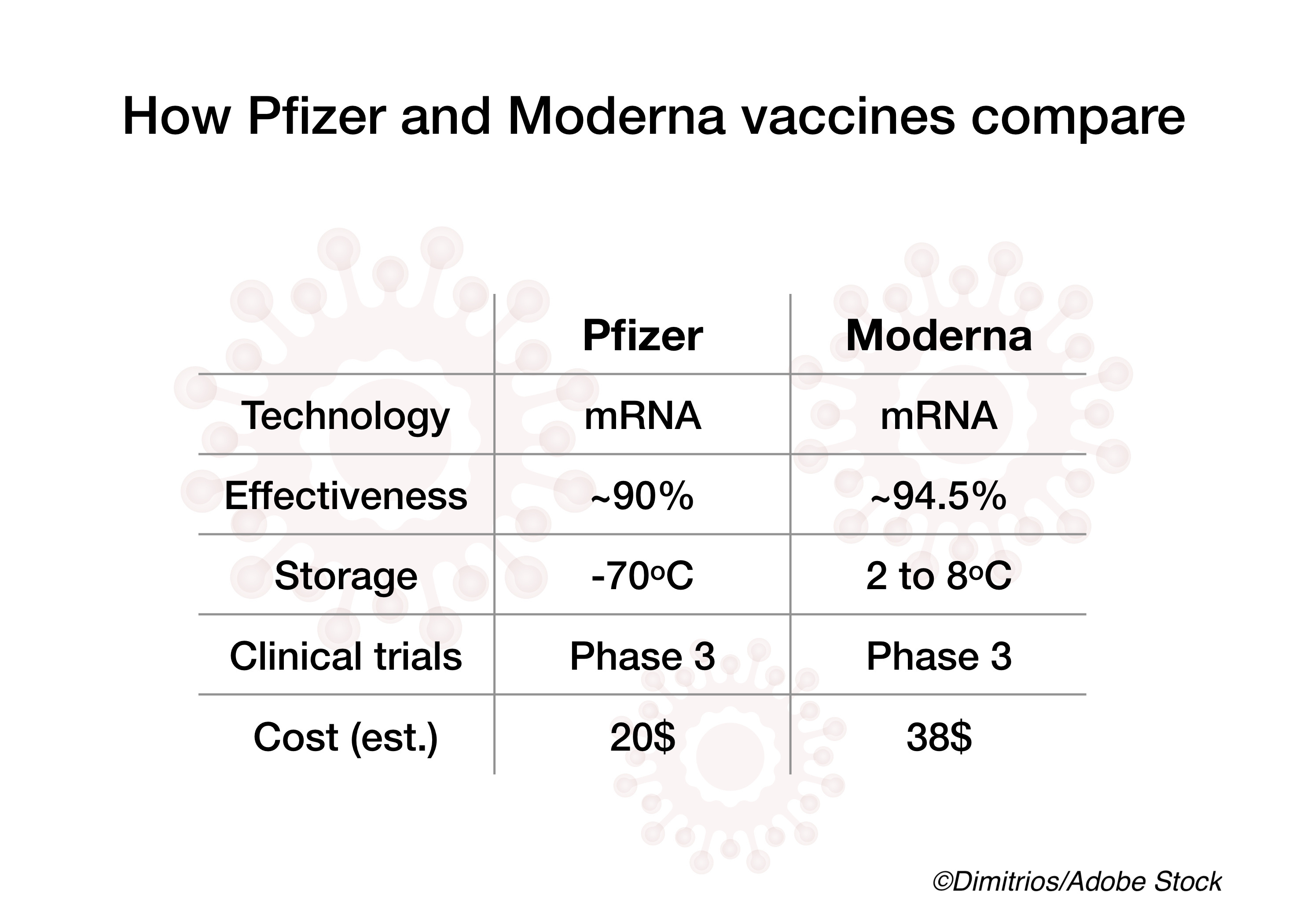
Early reports from the U.S. and Israel on two mRNA-based Covid-19 vaccines, Pfizer/BioNTech’s BNT162b2 and Moderna’s mRNA-1273, suggest that the two vaccines are not only safe but also effective.
In one report published in Morbidity and Mortality Weekly Report, the CDC provided an overview of U.S. safety monitoring for both vaccines — and, fortunately, the results seem promising so far.
“CDC conducted descriptive analyses of safety data from the first month of vaccination (Dec. 14, 2020–Jan. 13, 2021),” wrote Julianne Gee, MPH, and colleagues from the CDC’s Covid-19 Response Team. “During this period, 13,794,904 vaccine doses were administered, and [Vaccine Adverse Event Reporting System] VAERS received and processed 6,994 reports of adverse events after vaccination, including 6,354 (90.8%) that were classified as non-serious and 640 (9.2%) as serious. The symptoms most frequently reported to VAERS were headache (22.4%), fatigue (16.5%), and dizziness (16.5%)… The initial post-authorization safety profiles of the two Covid-19 vaccines in current use did not indicate evidence of unexpected serious adverse events. These data provide reassurance and helpful information regarding what health care providers and vaccine recipients might expect after vaccination.”
Also, during the study period, CDC had 62 confirmed reports of anaphylaxis following vaccine administration — 46 (74.2%) for the Pfizer/BioNTech shot and 16 (25.8%) for the Moderna shot. However, the report authors explained that the rate of anaphylaxis for Covid vaccines (4.5 cases per million doses administered) was within the range reported for other vaccines, including inactivated influenza vaccine (1.4 per million), pneumococcal polysaccharide vaccine (2.5 per million), and live attenuated herpes zoster vaccine (9.6 per million).
VAERS also received reports of 113 deaths post-vaccination, but Gee and colleagues noted that “available information from death certificates, autopsy reports, medical records, and clinical descriptions from VAERS reports and health care providers did not suggest any causal relationship between Covid-19 vaccination and death.”
“No unexpected patterns of reactions or other safety concerns have been identified during early monitoring,” the report authors concluded. “CDC and FDA will continue to monitor the safety of Covid-19 vaccines to inform vaccination policy and to maintain public confidence.”
Meanwhile, a Lancet Correspondence from Israel assessing the efficacy of BNT162b2 found that the vaccine led to substantial early reductions in SARA-CoV-2 infection and symptomatic Covid-19 rates after administration of the first vaccine dose, offering support for delaying the second dose in cases where vaccines are in short supply.
For their report, Eyal Leshem, MD, and colleagues from the Sakler Faculty of Medicine at Tel Aviv University in Tel Aviv, Israel, analyzed a retrospective cohort of 9,109 vaccine-eligible health-care workers (HCWs) to compare vaccine-associated Covid-19 rate reductions against unvaccinated controls.
By Jan. 24, 2021, 7,214 (79%) of their cohort had received a first vaccine dose and 6,037 (66%) had received a second dose.
“Overall, there were 170 SARS-CoV-2 infections among HCWs in the period between Dec 19, 2020, and Jan 24, 2021, of which 99 (58%) HCWs reported symptoms and were designated as Covid-19 cases [HCWs with symptomatic infection],” they found. “Of the 170 HCWs who became infected, 89 (52%) were unvaccinated, 78 (46%) tested positive after the first dose, and three (2%) tested positive after the second dose.”
Leshem and colleagues reported that, compared with a SARS-CoV-2 infection rate of 7.4 per 10,000 person-days in unvaccinated HCWs, rates of infection were 5.5 per 10,000 person-days 1-14 days after the first vaccine dose (adjusted rate reduction: 30%; 95% CI 2-50) and 3.0 per 10,000 person-days 15-28 days after first dose (adjusted rate reduction: 75%; 95% CI 72-84). And, compared to a symptomatic infection rate of 5.0 per 10,000 person-days in the unvaccinated, symptomatic disease rates were 2.8 (adjusted rate reduction: 47%; 95% CI 17-66) and 1.2 (adjusted rate reduction: 85%; 95% CI 71-92) per 10,000 person-days on days 1-14 and days 15-28 after the first dose, respectively.
These early reductions in SARS-CoV-2 infections and symptomatic disease rates “provide support of delaying the second dose in countries facing vaccine shortages and scarce resources, so as to allow higher population coverage with a single dose,” Leshem and colleagues wrote; however, they noted that longer follow-up to assess long-term efficacy of a single vaccine dose is necessary to inform a second dose delay policy.
John McKenna, Associate Editor, BreakingMED™
Cat ID: 190
Topic ID: 79,190,791,932,730,933,190,926,192,927,151,928,925,934