

According to current estimates, more than 350,000 people experience sudden cardiac death in the United States each year. Patients with low ejection fraction (EF) are at risk for sudden cardiac death, and clinical trials have established that implantable cardioverter-defibrillators (ICDs) improve survival for these individuals. Guidelines recommend ICDs as primary prevention for patients with an EF of 35% or lower if they do not improve after being treated with optimal medical therapy for at least 40 days after a myocardial infarction (MI).
Studies suggest that ICDs are underutilized in routine clinical practice, especially after a patient suffers an MI. The incidence of MI and the resulting sequelae from these events increase with age. The benefit of ICDs as primary prevention is controversial among older patients because this population is underrepresented in clinical trials. Clinicians may be uncertain about the efficacy of ICDs in an older patient population and must also consider treatment goals and procedural risks. These factors may discourage the use of ICDs among older adults.
A Closer Look
In a retrospective study published in JAMA, Sean D. Pokorney, MD, MBA, and colleagues examined data from Medicare beneficiaries with an EF of 35% or less after MI. Participants were treated at 441 U.S. hospitals between 2007 and 2010, but were excluded if they had a prior ICD implant. The investigators evaluated the incidence and hospital variation of 1-year ICD implantation after MI among potentially eligible patients. They also examined factors that were linked to 1-year ICD implantation and compared 2-year mortality between patients with and without ICDs.
The study was unique in that it evaluated the use and timing of ICD implantation in the post-MI setting. By using a large, national acute MI registry linked to Medicare data, the analysis addressed an understudied older-aged population that is at high risk of cardiac adverse outcomes but is often undertreated. “Our intent was to identify opportunities to optimize the consideration and use of ICDs after older patients had an MI,” adds Dr. Pokorney.
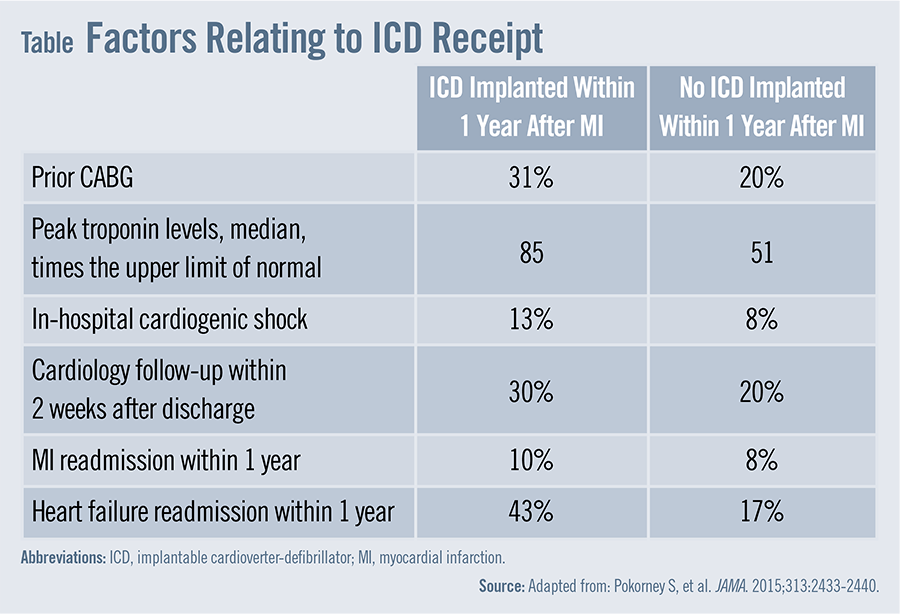
According to the study results, the cumulative 1-year ICD implantation rate among more than 10,000 older MI patients with an EF of 35% or lower was 8.1%. “This means that less than one in 10 Medicare patients with a low EF after an acute MI received an ICD within a year of their hospital discharge,” says Dr. Pokorney. Patients who received ICDs were more likely to have prior CABG procedures, higher peak troponin levels, in-hospital cardiogenic shock, and cardiology follow-up within 2 weeks after discharge when compared with those who did not receive an ICD within 1 year (Table).
The analysis also revealed that study patients who received an ICD had lower 2-year mortality rates than those who did not receive an ICD. The 2-year mortality rate was 15.3 events per 100 patient-years for those receiving ICDs, compared with 26.4 events per 100 patient-years for those not receiving the devices. These findings remained after adjusting for differences in baseline characteristics, in-hospital revascularization status, and post-discharge MI or heart failure readmissions.
“We also found that patients who had more contact with the healthcare system—with early cardiology follow-up or readmissions for MI or heart failure—had a higher likelihood of ICD implantation,” Dr. Pokorney says. “Patients with recurrent heart failure and recurrent MI were also more likely to get ICDs.”
Consider Perceptions
Previous research has shown that older patients have lower rates of ICD use than their younger counterparts. This may be due to the perception that older patients derive less benefit from ICDs. The study showed that patients who have these characteristics and do not receive an ICD had a 1.7-fold higher proportion of death. The magnitude of this association is consistent with the relative risk reductions that have been seen in other research.
Tailor Approaches
Individualized shared decision making is critical because ICD therapy may shift death from a sudden event to a more gradual and comorbid process. “We need to take into account each patient’s quality of life, treatment goals, and preferences,” Dr. Pokorney says. “Our data suggest that age alone should not be considered a contraindication when considering candidates for ICDs.”
Additional research is needed to determine evidence-based approaches that can increase rates of ICD implantation among eligible patients. “Close clinical follow-up is necessary to optimize medical therapy prior to implanting ICDs,” says Dr. Pokorney. “Transitions in care after MI are points of vulnerability that may be helped with quality improvement interventions. Systematic interventions must be developed to encourage close outpatient follow-up, improve communication and implementation of long-term care plans, and enhance patient education. Such interventions may help us identify more effective ways to optimize ICD use among older patients.”
 PWeekly
PWeekly
{kind=link}