

About 80,000 lower-extremity amputations (LEAs) are performed each year on patients with diabetes in the United States. Statistical analyses have shown that the annual incidence of LEA in older patients with diabetes was 5.0 per 1,000 in 2006-2007, but decreased to 4.0 per 1,000 in 2008. “While the downward trend is encouraging, it’s important to also analyze variations in the rates of LEAs throughout the country,” says David J. Margolis, MD, PhD.
Previous studies have shown that there appears to be geographic variation in the incidence of LEAs among Medicare beneficiaries with diabetes. Furthermore, about $52,000 is reimbursed annually for a Medicare beneficiary with diabetes and an LEA. “By learning more about geographic variation in LEA, we can then identify causes and develop targeted interventions for prevention,” Dr. Margolis says.
Assessing Geographic Variation of LEAs
In the November 2011 issue of Diabetes Care, Dr. Margolis and colleagues conducted a study to explore graphic variation of incident LEAs among Medicare beneficiaries with diabetes. The investigators performed a study of the full population of Medicare beneficiaries because it is, in essence, the largest healthcare insurance provider in the U.S. and the largest government-funded medical entitlement program. The geographic unit of analysis was hospital referral regions (HRRs). The study then evaluated the incidence of LEA by HRRs as a function of geographic location throughout the country. Other items analyzed in the study included sociodemographic factors, risk factors for LEA, diabetes severity, provider access, and cost of care.
“Our findings showed that rates of amputation varied greatly according to where patients lived, but questions remain as to why this occurs,” says Dr. Margolis. “While previous studies have suggested that rates of amputation may be declining among Americans with diabetes, our analysis suggests that LEA rates can be almost double the national average among older Americans in some parts of the U.S.”
“By learning more about geographic variation in LEA, we can then identify causes and develop targeted interventions for prevention.”
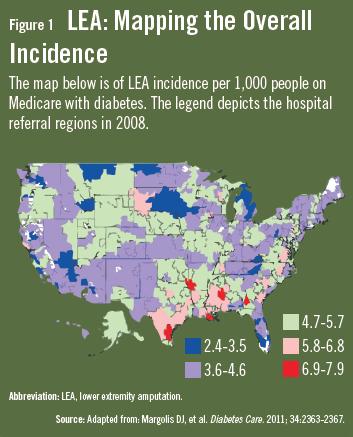
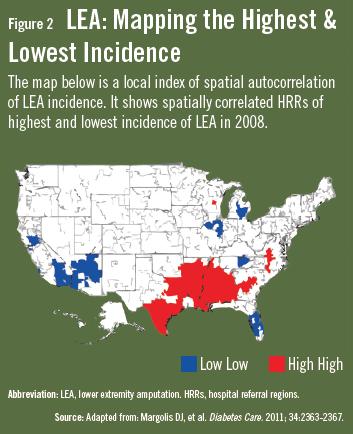
The incidence of LEA was highly concentrated in neighboring HRRs. In 2008, disproportionately high rates of LEA existed in certain pockets of southeast Texas, southern Oklahoma, Louisiana, Arkansas, and Mississippi (Figure 1 & Figure 2). For these locations, the LEA rate ranged from 7.0 to 8.0 per 1,000. “These findings are important, considering the national rate that same year was 4.5 per 1,000,” Dr. Margolis adds. “On the other hand, we observed disproportionately low rates of LEA throughout southern Florida as well as parts of New Mexico, Arizona, and eastern Michigan. In these spots, Medicare beneficiaries with diabetes had amputations at a rate of 2.4 to 3.5 per 1,000.”
Dr. Margolis notes that accounting for geographic location greatly improved the researchers’ ability to understand the variability in LEA. Additionally, covariates associated with LEA per HRR included:
Socioeconomic status.
Prevalence of African Americans.
Age.
Diabetes.
Mortality rate associated with having a foot ulcer.
Interpreting Findings of LEA prevalence
Dr. Margolis and colleagues were able to account for the prevalence of diabetes in a given area, the number of people diagnosed with diabetic foot ulcers, and an area’s socioeconomic status. However, these factors accounted for some of the geographic variation, but not all of it. It is also important to note that the relatively high rates of LEA in certain regions do not necessarily mean that the rates are too high, Dr. Margolis says.
“It’s possible that physicians in areas of high rates of LEA see more people with severe diabetes complications,” explains Dr. Margolis. “Based on their experiences, they may believe that an earlier amputation correlates with better outcomes. Currently, the decision to perform LEA is not clear-cut. Furthermore, there are no general guidelines on when amputations should be performed in individuals with severe diabetic ulcers. This means the decision for LEA relies on physician judgment and patient preference.”
More Research Needed on LEA Variations
Considering the results of the investigation, Dr. Margolis believes more research is needed to better understand the reasons for geographic variations with LEA in Medicare beneficiaries with diabetes. “Ideally, we want to look more closely at the areas of high and low LEA rates in an effort to determine the causal factors. Doing so will enable researchers to target interventions to further reduce the rate of LEAs. This will require gathering data on clinician education in LEA, the role of patient preferences, and information on genetic risk factors that predispose patients to LEA. Until these data emerge, clinicians should strive to help people with diabetes take the necessary steps to protect their limbs.”
 Janine Anthes
Janine Anthes
{kind=link}
{kind=link}