

In 2010, I blogged about CT scan being the gold standard for the diagnosis of appendicitis. Research over the last few years has confirmed what I wrote back then.
A recent example is this study of 11,841 patients who underwent appendectomy in 2016; 93.9% underwent one or more imaging studies. The overall rate of removing what turned out to be a normal appendix was 4.5%.
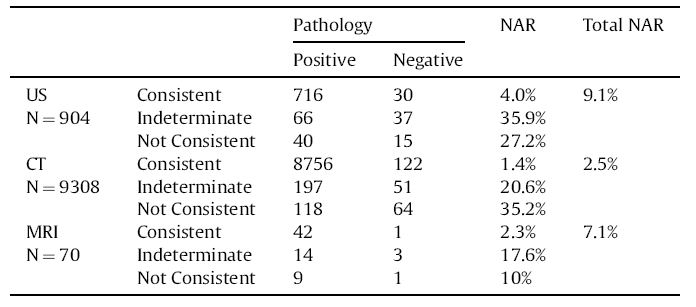
When a CT scan was used as the sole imaging study and the reading was consistent with the diagnosis of appendicitis, a normal appendix was removed only 1.4% of the time. Adding indeterminate and “not consistent with appendicitis” CT scan readings to the totals resulted in a negative appendix rate of 2.5%.
The table below shows the comparison of CT scan positive and negative pathologic findings to those of ultrasound and MRI.
The negative appendix rate for 719 patients who had no preoperative imaging studies was 26.2%.
The chance of having a negative appendix was significantly associated with female sex, smokers, those with no imaging studies, and those having ultrasounds. A reduced risk of having a negative appendectomy was associated with patients who had the systemic inflammatory response syndrome or sepsis, an elevated white blood cell count, or a preoperative CT scan.
Both an ultrasound and a CT scan were obtained in 866 patients. The addition of a CT scan markedly improved the rate of finding appendicitis for ultrasound readings consistent with appendicitis, indeterminate, or not consistent with appendicitis.
The authors wrote, “if an imaging study is inconclusive, there may be additional value in obtaining a different scan to improve diagnostic accuracy.”
A radiologist colleague, @RogueRad, and I addressed the overblown risks of CT scan radiation in a 2016 blog post.
Some other diagnostic modalities are white blood cell count, C-reactive protein (CRP) blood test and the Alvarado score.
UpToDate states that WBC had a sensitivity (true positive rate) of 0.84 and a specificity (true negative rate) of 0.67 compared to CRP with an 0.81 sensitivity and a 0.54 specificity. Although the combination of WBC and CRP had a higher sensitivity of 0.93, the specificity of the combination of tests was only 0.62, far below the 0.96 specificity of CT scan which has a sensitivity of 0.96 as well.
This led the authors of the UpToDate section on appendicitis to state “no WBC count or CRP level can safely and sufficiently confirm or exclude the suspected diagnosis of acute appendicitis.”
The Alvarado score can be useful to rule out appendicitis if the score is 0 to 3, but the recommendation is to evaluate such patients for other causes of abdominal pain (for which CT scan is very good). A 2016 review of diagnostic measures in appendicitis found in 30 studies of both adults and children, the sensitivity of the Alvarado score was 0.77 and the specificity was 0.79.
Paraphrasing what I said in 2010 regarding the use of CT scanning—do you want an accurate diagnosis for yourself or your child with the theoretical but unproven increased risk of radiation-induced cancer years later or would you decline CT scanning and accept a higher rate of normal appendix removal? Based on a study of children with head trauma whose parents overwhelming agreed to CT scanning, I think most people would choose the former.
Skeptical Scalpel is a retired surgeon and was a surgical department chairman and residency program director for many years. He is board-certified in general surgery and a surgical sub-specialty and has re-certified in both several times. For the last 8 years, he has been blogging at SkepticalScalpel.blogspot.com and tweeting as @SkepticScalpel. His blog has had more than 3,000,000 page views, and he has over 19,000 followers on Twitter.
 SkepticalScalpel
SkepticalScalpel