

Pain is one of the most common reasons for patients seeking care in EDs, accounting for up to 42% of all emergency room visits. Emergency physicians vary widely in prescribing patterns and often have difficulty assessing patients’ level of pain. There may also be reluctance to provide pain medications due to concerns that patients are trying to obtain prescription drugs for non-therapeutic purposes. “These individuals— who are often labeled as drug-seeking—are a difficult group of patients to manage in the ED,” says Casey A. Grover, MD. “They often present to the ED with conditions that are difficult to evaluate, and may also engage in deceptive behaviors in an effort to fool clinicians into giving them additional medications.”
It is estimated that up to 20% of all ED visits may be due to drug-seeking behavior. “Drug-seeking patients have been known to use large amounts of medical resources,” says Dr. Grover. “They may occupy beds in EDs that would be more appropriately used for people truly in need of emergency care.”
Prescription drug abuse and misuse is a growing epidemic throughout the United States, and more and more emergency physicians are encountering drug-seeking patients in daily practice. “Despite the magnitude of the problem,” Dr. Grover says, “there is still much to learn about these patients, their patterns, and how best to manage them.”
Intriguing New Data on Drug-Seeking Behavior
Studies have been conducted on screening tools to identify drug-seeking behaviors in chronic pain patients, but few have provided quantitative data on such behaviors in the ED. With this in mind, Dr. Grover and colleagues performed a case-control study examining the relative frequency of various drug-seeking behaviors in drug-seeking patients as compared with all ED patients. The study was published in the January 2012 Journal of Emergency Medicine. “Our goal was to provide emergency physicians with information as to which drug-seeking behaviors are most commonly used by drug-seeking patients,” says Dr. Grover. “Identifying behaviors that are most commonly used by drug-seeking patients may help evaluations of patients suspected of drug-seeking behavior.”
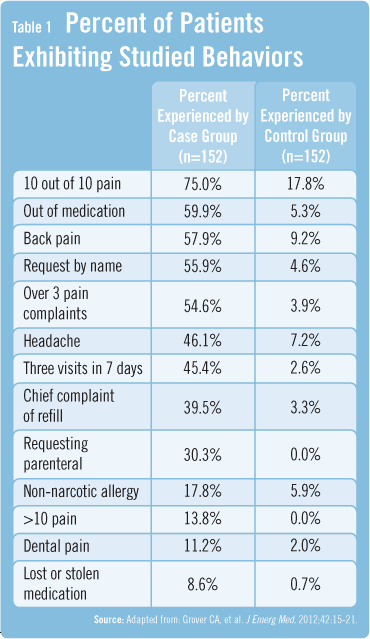
A retrospective chart review of 152 drug-seeking patients and of age- and gender-matched controls was conducted, with the authors noting several drug-seeking behaviors that were exhibited over 1 year. Drug-seeking patients accounted for 2,203 visits to the ED, averaging about 14.5 visits per patient per year. For the control group, patients accounted for 315 visits to the ED, which is an average of 2.1 visits per patient per year. Patients in the drug-seeking arm reported their pain level as 10 out of 10 more often than control group patients (Table 1). Additionally, drug-seeking patients occasionally complained of pain levels greater than 10 out of 10, while the control group had no instances of these events. Drug-seeking patients were also significantly more likely to request medications parenterally.
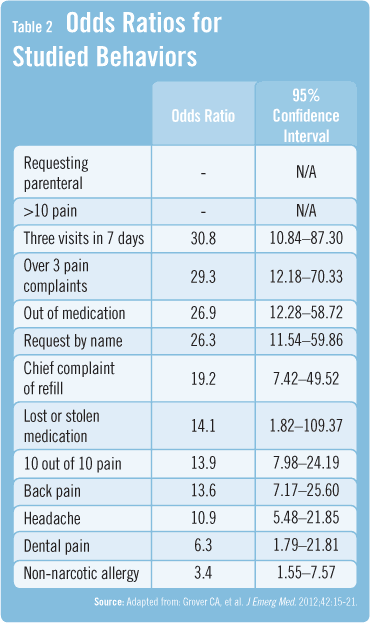
The odds ratios for both requesting parenteral medication and reporting pain levels greater than 10 out of 10 were significantly higher than all others observed in the study (Table 2). These were the most predictive of drug-seeking behavior, while a non-narcotic allergy was less predictive. However, the odds ratio for a non-narcotic allergy was greater than 1, and was still a behavior that was more commonly used by drug-seeking patients than the control group. For other studied behaviors, the confidence intervals were too wide to allow the authors of the study to meaningfully interpret the data.
Challenges Remain in Deciphering Pain
According to Dr. Grover, chronic narcotic use can make patients more sensitive to pain. “These individuals may truly be suffering from the most severe pain possible. On the other hand, patients with narcotic abuse and dependency often exaggerate pain complaints in order to get their desired medication. Chemical dependency can become a major motivating factor for patients to seek emergency care. Unfortunately, it’s nearly impossible to definitively determine if they’re seeking care in an attempt to get medications for non-therapeutic reasons.” The current literature on drug-seeking patients consists largely of small studies, according to Dr. Grover, and larger-scale studies are needed. “These efforts will hopefully help us gain a better overall picture of the frequency of these behaviors and eventually help us establish strategies to optimize how we manage drug-seeking patients.”
 Janine Anthes
Janine Anthes
{kind=link}
{kind=link}