
CKD affects more than 37 million adults in the United States and drives nearly $120 billion in Medicare costs annually. Understanding the interplay between CKD detection, disease progression, and healthcare spending is critical to informing policies that promote better CKD management, both clinically and economically.
In a white paper published by Milliman, my colleague, Rebecca Smith, MBA, and I sought to understand how patients’ rates of disease progression, healthcare utilization, and costs empirically change across distinct stages of CKD. We analyzed 2014-2018 commercial and Medicare fee-for-service (FFS) administrative claims and identified patients in various CKD stages. We then tracked patients’ disease progression, healthcare use, and total costs of care (TCOC) throughout the study period.
Early-Stage CKD Is Undercoded in Claims Data
We found that that early-stage CKD (stages 1-2) is under coded in claims data. According to the National Health and Nutrition Examination Surveys (NHANES), 4.7% of US adults have CKD stage 1 and 3.4% have CKD stage 2. However, we identified only 0.8% of patients in stage 1 and 0.7% in stage 2, across both commercial and Medicare populations.
Numerous factors contribute to CKD under coding. Current preventive guidelines from the U.S. Preventive Services Task Force do not encourage screening for CKD in certain asymptomatic adults, while national health plan quality metrics, such as the Healthcare Effectiveness Data and Information Set, do not promote kidney health evaluations among all high-risk groups. Furthermore, early-stage CKD diagnoses are not leveraged by predictive models used for health plan risk adjustment. Therefore, plans are unlikely to promote early testing, as it does not improve compensation. As a result, many patients who could benefit from proactive management are not being identified until they reach more severe and costly stages of disease.
There is a clear acceleration in disease progression between CKD stages 3 and 4. While patients in stages 4 and 5 are 40% to 46%, respectively, more likely to progress to higher disease stages within 1 year, patients in stages 1 to 3 are only 19% to 25%, respectively, more likely to do so, translating to1.5 to 2.0 times greater likelihood of such progression (Figure 1).
Healthcare Costs Increase Exponentially
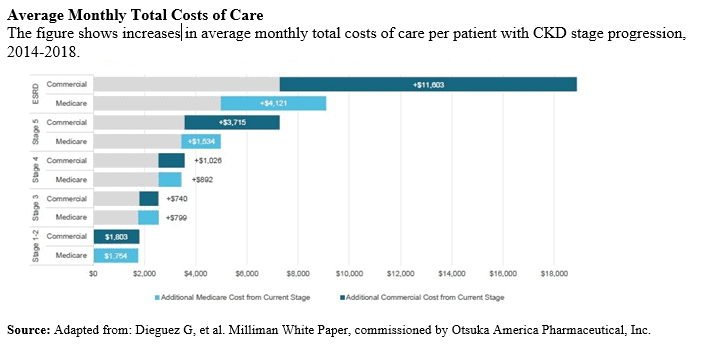
As their CKD advances, patients’ overall healthcare costs increase exponentially. Patients with commercial insurance incurred average monthly TCOC that climbed from $1,803 in stages 1-2 to $7,284 in stage 5. TCOC more than doubles, reaching $18,887 per month, for patients with end-stage renal disease (ESRD). We observed a similar pattern in the Medicare population, where average costs peaked at $9,099 per month for patients with ESRD (Figure 2).
These findings suggest early detection and intervention, if able to delay disease progression, could significantly reduce dialysis dependency, demand for kidney transplants, and healthcare costs for patients with Medicare FFS or commercial insurance. Real-world clinical studies have linked longer nephrology care before ESRD with better outcomes. Yet, patients often remain undiagnosed until their disease has progressed to more rapidly advancing stages, at which point patients’ likelihood of further disease progression has nearly doubled.
Effective early interventions are available and critical to implement, but additional research may be needed to identify potential barriers to their use. Changes to kidney-related screening guidelines and quality metrics have the potential to drive early detection and intervention. It is equally important that payers also be incentivized to drive early-stage diagnosis and treatment via inclusion of earlier stages of CKD in risk score models. These changes would be influential to payers and healthcare professionals managing kidney care costs.
 Physician's Weekly Admin
Physician's Weekly Admin

{kind=link}