

Clinicians should be aware of differences between male and female patients with psoriasis, how the disease manifests and how treatment should be approached.
With psoriasis, differences in disease manifestation and treatment outlook and goals exist between male and female patients using systemic agents, including conventional system agents (CSA) and tumor necrosis factor inhibitors or ustekinumab (TNFi/UST). However, few studies have addressed sex differences as they pertain to systemic agent use, such as CSA discontinuation and switch from CSA to TNFi/UST.
Past research has shown that female patients have higher expectations for achieving treatment goals than male patients. Female patients anticipate faster skin improvement and a return to normal life, even though male patients may present with more severe psoriasis. These differences in psoriasis severity and treatment goals between male and female patients may determine how clinicians manage their treatment. Female patients, for example, may discontinue treatment prematurely or request a treatment change if their skin clearance is slower than expected.
Similar Rates Observed for Both Male and Female Patients
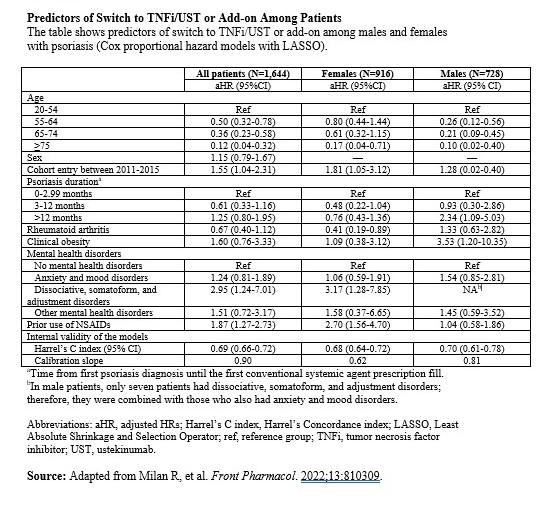
For a paper published in Frontiers in Pharmacology, my colleagues and I utilized a health administrative database to examine sex differences in patterns of CSA use and determine factors linked with switching to (or adding) a TNFi/UST. Our retrospective cohort study included 1,644 patients with psoriasis (mean age, 61; 55.7% female) who started a CSA between 2002 and 2015. The study team used Cox regression models with the Least Absolute Shrinkage and Selecting Operator (LASSO) to identify socioeconomic and clinical characteristics that predicted switch/add-on TNFi/UST.
We observed similar rates for switch and add-on of TNFi/UST between male and female patients with psoriasis. However, most predictors of switch/add-on were sex-specific. For example, among males, we found an increased risk for longer psoriasis disease duration and obesity by at least 2.3-fold. Among female patients, prior use of NSAIDs and the presence of certain mental health disorders increased the risk for switch/add-on by 2.7-fold. Interestingly, female patients with rheumatoid arthritis (RA) as a comorbidity had a 60% reduced risk for switch/add-on (Table).
A Need Exists to Improve Access to Biologic Agents
Our findings may help clinicians improve the management of male and female patients with moderate-to-severe psoriasis in need of systemic agent treatment. Since most countries with a universal healthcare system reimburse biologic agents only for patients who do not respond well to CSA or among whom CSA are contraindicated, a need exists to improve access to biologic agents. For male patients with obesity and for those who have lived with psoriasis for an extended time, and for female patients who experience pain or mental health symptoms, treatment with biologic agents may save them the burden of going through a failed treatment experience and help improve their psoriasis outcomes faster, especially since biologic agents are known for being more effective than CSA.
My colleagues and I also included variables related to psoriasis treatments such as the type of initial CSA received, the specialty of the prescriber, and prior use of topical agents and phototherapy. However, none of these variables were selected by our model, thus possibly indicating that the decision of the healthcare professional to prescribe a biologic agent among male and female patients with psoriasis was mostly based on patients’ clinical profiles and not on these factors.
Larger Studies Focusing on Psoriasis Severity Are Needed
We were surprised to find that psoriatic arthritis (PsA) was not associated with a risk for switch in both male and female patients, while RA was linked with a decreased risk for switch among female patients. Since PsA and RA are immune-mediated conditions for which biologic agents can also be prescribed, additional research is warranted to better understand the reduced risk for switch/add-on of TNFi/UST among female patients with both psoriasis and RA.
Additionally, larger studies, specifically those focused on psoriasis severity, are needed to confirm our findings and their impact on clinical practice and provincial drug policy. Larger studies will also allow comparisons between individual CSAs and the assessment of predictors of switch to TNFi/UST and those for receiving these agents as add-on, separately.
 Martta Kelly
Martta Kelly
{kind=link}