

The incidence of physician-diagnosed gout has risen over the past 20 years and now affects about 8.3 million adults in the United States. Uric acid excess has been identified as the key contributor to gout. When hyperuricemia develops, crystals containing the salt of uric acid can form and deposit in joints, causing pain and swelling that can be debilitating for patients and adversely affect quality of life. Published research has indicated that gout may be attributed to excess uric acid promoted by several comorbidities, including hypertension, obesity, metabolic syndrome, type 2 diabetes, and extensive treatment with thiazide and loop diuretics for cardiovascular disease.
Important New Guidelines on Gout
To improve patient care, the American College of Rheumatology (ACR) published evidence-based guidelines for managing gout in Arthritis Care & Research. A U.S. expert task force was convened to develop two guidelines, the first focusing on systematic non-pharmacologic and pharmacologic therapeutic approaches to hyperuricemia, and the second covering therapies and prophylactic anti-inflammatory treatments for acute gouty arthritis. The guidelines provide recommendations based on medical literature spanning from the 1950s to the present.
“These guidelines promote greater awareness of the need for urate control and the increasing burden and prevalence of gout,” says Robert A. Terkeltaub, MD, who was senior author on both ACR guidelines. “The intent is to educate physicians on effective ways to prevent gout attacks and provide them with recommendations for using therapies and diet and lifestyle measures for long-term care.”

Hyperuricemia
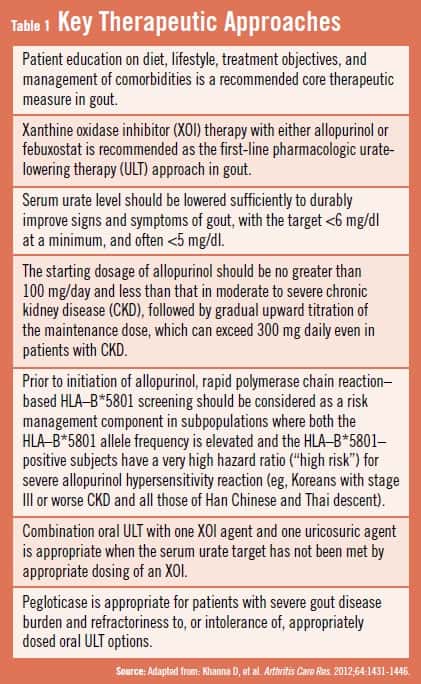
According to the guidelines, initial measures for treating gout should include patient education about the role of uric acid in the disease and non-pharmacologic approaches. “Patients should be educated on diet, lifestyle choices, treatment objectives, and management of concomitant diseases,” says Dr. Terkeltaub. “However, most patients with recurrent attacks won’t achieve adequate relief of symptoms with lifestyle efforts alone, meaning pharmacotherapy will likely be necessary.”
A key aspect of initial treatment decision making is to identify patient comorbidities. In addition, recognition of potential drug interactions and how some medications influence serum urate levels is important. “To improve gout symptoms, the ACR recommends that target serum urate levels be below 6 mg/dL at a minimum, but that threshold may need to be below 5 mg/dL in many patients, depending on comorbidities,” explains Dr. Terkeltaub.
Several treatments are indicated as first-line urate-lowering therapy, including xanthine oxidase inhibitors (eg, allopurinol) or febuxostat, a newer agent that has recently reached the market (Table 1). The guidelines also provide specific information on allopurinol, recommending that the initial dose of this therapy be no greater than 100 mg/day; the dose should be less for patients with chronic kidney disease (CKD). This should then be followed by a gradual increase of the maintenance dose, which can exceed 300 mg, even in those with CKD. Other recommendations address screening of high-risk patients for allopurinol allergy (eg, Han Chinese, Thai, and Koreans) before using allopurinol, and appropriate strategies for when to prescribe combination urate lowering therapy.
Acute Gouty Arthritis
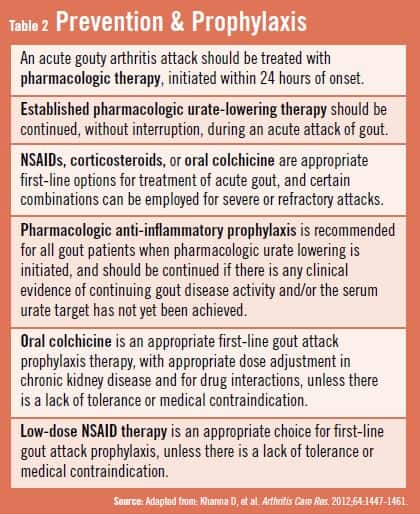
The ACR guidelines also give recommendations for using therapies and prophylactic anti-inflammatory treatment for acute gouty arthritis (Table 2). They stress initiating pharmacologic therapy within 24 hours of onset of acute gouty arthritis attacks and continuing urate-lowering therapy (ULT) without interruption during acute gout flares. Dr. Terkeltaub says “several options are available, depending on symptom severity, usually with monotherapy as the initial approach.”
The ACR also offers guidance on the optimal use of NSAIDs, corticosteroids, or oral colchicine as first-line treatment for acute gout and on the use of combinations of these medications for severe or unresponsive cases. Oral colchicine or low-dose NSAIDs can be used as first-line therapy to prevent attacks when initiating ULT, provided there are no contraindications or issues with lack of tolerance.
Looking Ahead for Effective Gout Treatment
“The long-term morbidity and impairment of health-related quality of life are now better recognized, particularly in gout patients with multiple comorbidities,” Dr. Terkeltaub says. “Along with educating patients about effective treatment, the ACR guidelines will hopefully improve adherence, quality of care, and management of gout. More research is needed to help us better understand how to optimize combinations of therapies and prophylaxis. Studies assessing cost of treatment, head-to-head comparisons of therapies, and analyses on patient preferences and long-term safety are also necessary to further decrease the burden of gout in the future.”
 admin
admin
{kind=link}
{kind=link}