

In 2011, the American Thoracic Society, the European Respiratory Society, the Japanese Respiratory Society, and the Latin American Thoracic Association published an evidence-based guideline on the diagnosis and management of idiopathic pulmonary fibrosis (IPF). Since that time, “a tremendous amount of new data on IPF treatment has accumulated, including phase III clinical trial results and newly available medications,” says Ganesh Raghu, MD, FACP, FCCP. “The societies felt it was time to update the guideline focusing on IPF treatment.” The updated guideline, which does not address IPF diagnosis, was published in the American Journal of Respiratory and Critical Care Medicine.
A New Landscape
According to Dr. Raghu, who chaired the guideline-writing committee, six studies were instrumental in the update. “The standard of care for IPF has been prednisone, azathioprine, and n-acetylcysteine triple therapy, based on a study published in 2005,” he says. “We gave a weak recommendation for this treatment in the 2011 guideline.” However, the PANTHER-IPF study found in 2012 that this triple therapy was harmful in patients with IPF, leading to higher mortality, more hospitalizations, and more serious adverse events when compared with placebo. Also, acetylcysteine monotherapy was found to have no significant benefit over placebo with respect to preserving forced vital capacity (FVC).
“The phase IIb nintedanib study, published as the TOMORROW trial showed that the drug had a positive effect on decreasing the rate of FVC decline, acute exacerbations, and quality of life in patients with IPF,” says Dr. Raghu. In May 2014, results of the INPULSIS-1 and INPULSIS-2 studies were published, showing that nintedanib reduced the decline in FVC and slowed disease progression in patients with IPF. In the same issue of the New England Journal of Medicine, the ASCEND trial results showed that pirfenidone reduced disease progression in patients with IPF when compared with placebo.
Since the 2011 guideline was published, study results also showed that warfarin had no benefit in patients with IPF and instead increased mortality. Ambristentan was shown to be harmful in patients with IPF, which lead to the FDA declaring that the drug not be used in patients with IPF, regardless of whether or not they also had pulmonary hypertension.
“These pivotal trials and the FDA approval and availability of pirfenidone and nintedanib have created a new landscape for patients with IPF,” Dr. Raghu adds.
Keep Recommendations in Context
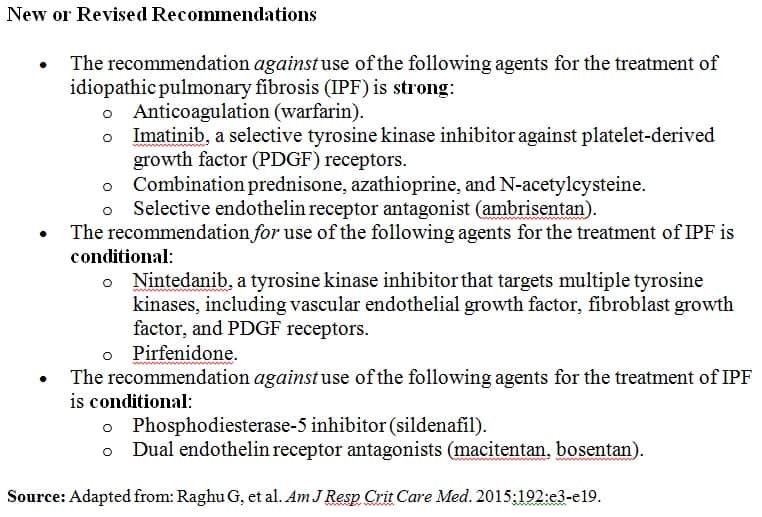
New and revised recommendations in the treatment section of the guideline were based on the aforementioned study results (Table). Conditional recommendations against the use of n-acetylcystein monotherapy for IPF and for the use of antacid therapy for IPF treatment remained unchanged from the 2011 guideline. The conditional recommendations for the use of pirfenidone, nintedanib, and antacid therapy should not be viewed as having similar strength,” cautionsDr. Raghu. “The evidence was much stronger for pirfenidone and nintedanib based on high-quality randomized clinical trials when compared with antacid treatment.
“Our recommendations should be considered in the context of individual patient values and preferences,” says Dr. Raghu. “They should not be viewed as absolute recommendations for all patients with IPF because clinical trials for these medications have not included all subgroups of IPF patients. We do not provide recommendations for one treatment regimen over another because there have been no head-to-head comparisons of these agents.”
Dr. Raghu also stresses the importance of shared decision making in determining the appropriate treatment for patients with IPF. “Patients should be informed on the study data for these medications, particularly with regard to adverse events and their effect on decreasing the rate of disease progression,” he says. “Whereas pirfenidone and nintedanib are both good anti-fibrotic drugs with similar effects on decreasing the rate of decline of FVC in disease progression, they have significant gastrointestinal side effects that need to be discussed with patients. There are many other caveats that clinicians should take into consideration, including confidence in effect estimates, treatment costs, and the feasibility of treatment.”
Looking Ahead
According to Dr. Raghu, there are a number of ongoing clinical trials that will come to fruition in the next few years that will require the IPF treatment recommendations to be updated. “For example, the use of monotherapy n-acetylcysteine for patients with IPF is not settled,” he says. “Studies have shown that n-acetylcysteine does not affect FVC as an endpoint, but there may be other important endpoints to consider.” Dr. Raghu also points to the need for long-term studies on the safety and efficacy of pirfenidone and nintedanib. In the meantime, clinicians can use the updated treatment recommendations to make the most appropriate treatment choices for patients with IPF based on shared decision-making with well-informed patients.
 PWeekly
PWeekly
{kind=link}