
Since care for diabetic foot ulcers is delivered by a wide range of healthcare professionals, from nurses working in primary care to specialized diabetes foot clinics, collecting population-based data on diabetic foot ulceration is notoriously difficult. Furthermore, epidemiological data on populations with diabetic foot ulceration collected from selected subpopulations is open to bias, hence the importance of unselected population-based data.
To address this issue, my colleagues and I conducted a national, population-based, cohort study of people with diabetes, with the aim of describing the incidence of foot ulceration and amputation-free survival associated with foot ulceration status. Our paper, which was published in Diabetes Care, focused on the occurrence of foot ulceration stratified by history of previous foot ulceration and by type of diabetes, for a period of nearly 6 years, from 2012 to 2017. We used the Scottish Care Information-Diabetes database (SCI-diabetes) of unselected people with diabetes, which included 233,459 people with diabetes who were alive on January 1, 2012, identified from the national population-based register. SCI-Diabetes also collects real-time data from various sources such as other primary care records, prescribing records, laboratory data, hospital admissions, and surgical data, among others. The population included 23,395 people with T1D and 210,064 with T2D.
Death More Common Than Amputations
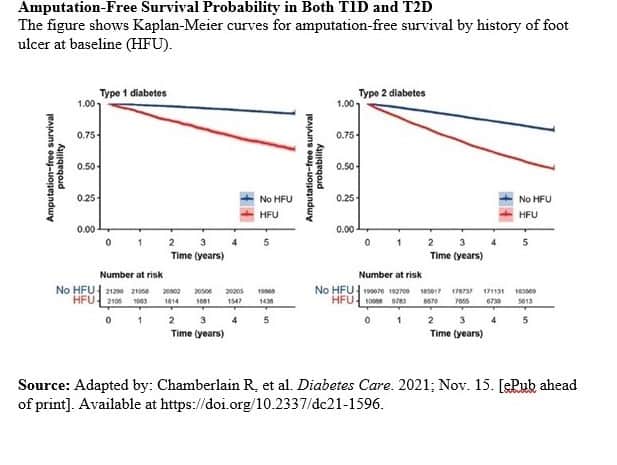
Our study team found that the overall annual incidence of foot ulceration was 11.2 per 1,000 person-years, with a rate of 7.8 per 1,000 person-years for a first-time ulcer. It is likely that some ulcers, especially those that healed quickly, may have been missed and so these estimations may be at the lower end of reality. Of patients who had experienced a previous ulcer, 34% developed a further foot ulcer, while 4% developed an ulcer for the first time during follow up. The rates of amputation-free survival are much worse in patients who have had a previous ulcer, with crude relative risks about five-fold for T1D and 2.5-fold for T2D (Figure).
{kind=link}
Overall, 21.7% of people either died or had an amputation during follow-up. We found that death occurred more often than amputation in both T1D (9.3% vs 2.1%) and T2D (22.3% vs 1.1%). Among patients with no history of foot ulceration, 19.6% died and 0.7% had an amputation; 20.1% had an event overall as some died after amputation. For people with a history of a foot ulcer, the corresponding figures were 44.5% (death), 9.4% (amputation), and 49.5% with an event overall.
Physical and Mental Risk Factors for Poor Outcomes
Risk factors for poor outcomes include well-recognized vascular and metabolic risk factors such as ischemic heart disease, stroke, peripheral vascular disease, renal failure, smoking, high blood pressure, and elevated cholesterol. In addition to these, mental illness, social deprivation, low BMI, and low A1C were risk factors, as low BMI and A1C are probable markers for frailty.
In conclusion, my colleagues and I found a strong association between a history of foot ulceration and amputation or death. After adjusting for all measured risk factors, previous ulceration was still associated with death or amputation, having a HR of 3.4 in T1D and 2.4 in T2D. However, our research, which focuses on the estimate of ulcer incidence in an unselected population-based national dataset, should help with healthcare planning and with workforce organization. Death remains the predominant adverse outcome for all groups in our study; therefore, aggressive cardiovascular risk factor modification is recommended. Finally, the emerging evidence regarding social deprivation, mental illness, and probable frailty as independent risk factors, warrants greater attention and future research should focus on interventions to improve outcomes.