

In March 2017, the American Society of Anesthesiologists issued the following guidelines regarding restriction of oral intake in infants, children, and adults undergoing elective surgery:
Clear liquids may be ingested for up to 2 hours before procedures requiring general anesthesia, regional anesthesia, or procedural sedation and analgesia.
A light meal or nonhuman milk may be ingested for up to 6 hours before elective procedures requiring general anesthesia, regional anesthesia, or procedural sedation and analgesia
Having once had an encounter with an anesthesiologist who postponed a case because my patient had a piece of hard candy in her mouth, I wanted to see how closely that guideline was being followed since its publication 2 years ago.
I posted a poll on Twitter. Although such polls are unscientific, over 3800 people responded, and the results are thought-provoking.
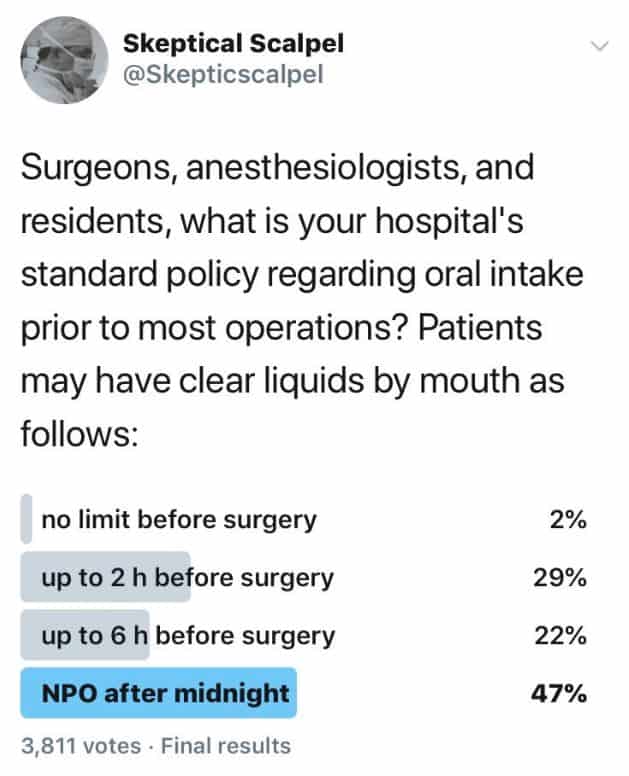
Almost half of those participating said their hospitals were still mandating that patients take nothing by mouth after midnight. A number posted comments describing their experiences and frustrations. Here are a few of them (edited for length and grammar).
“Our scheduled C-section patients are instructed to be completely NPO for 8 hours, including clears. I’ve even heard someone tell a patient they can’t chew gum because that increases how much saliva they swallow.” [Maybe patient should be issued “spittoons” so they could keep that tiny amount of saliva out of their stomachs.]
Many comments were about irrational case cancellations because of gum and candy such as this one by a gastroenterologist, “Literature says 2 hours for clears. However, our hospital anesthesiologists will cancel the case on a whim. Depends on their case load and how much they want to work. Had a case cancelled for chewing gum. As if I’m not suctioning their stomach out in real time, live, on camera!”
Here’s my favorite. “I once had an anesthesiologist cancel a case because the patient brushed their teeth in the am!” [I don’t know about you, but I try not to swallow any toothpaste. Even if someone did swallow toothpaste it is probably no more than a few milliliters of fluid.]
As recently as July 2018 at a well-known Boston area hospital, a 14-year-old boy was allowed nothing by mouth after midnight for an operation scheduled for 4 PM that day.
An anesthesiologist said, “The results of this poll are a little mind-boggling to me. [The ASA] guidelines dictate clears 2 hours before surgery is fine. How is the poll showing that patients have to be NPO for clears after midnight?”
This is not only about how patients feel. According to a 2017 review in the journal BJA Education, “Preoperative carbohydrate loading modifies insulin resistance, improves patient comfort and well-being, minimizes protein losses, and improves postoperative muscle function.” It also reduces hospital length of stay and does not increase the risk of aspiration.
In 2018, three European anesthesiology societies recommended a 1 hour fluid restriction for children undergoing anesthesia.
A 2017 European Journal of Anesthesia study of 11,500 patients from the UK found statistically significant reductions in postoperative nausea and vomiting when patients were allowed to have unrestricted clear fluids until the time of elective surgery.
I should be surprised by the poll’s results, but I’m not. One paper on the topic said it can take as long as 17 years for research findings to be incorporated into clinical practice. We will probably still have lots of thirsty patients for several more years.
Skeptical Scalpel is a retired surgeon and was a surgical department chairman and residency program director for many years. He is board-certified in general surgery and a surgical sub-specialty and has re-certified in both several times. For the last 8 years, he has been blogging at SkepticalScalpel.blogspot.com and tweeting as @SkepticScalpel. His blog has had more than 3,000,000 page views, and he has over 19,000 followers on Twitter.
 SkepticalScalpel
SkepticalScalpel