

“Clinicians who treat patients with osteoarthritis share a common perception that patients with knee osteoarthritis (OA) have better outcomes from exercise than those with hip OA,” explains Ewa M. Roos, PhD. “The reasoning may have to do with anatomical differences, such that the muscles in the knee are suspected of playing a greater role in stabilizing joints than those in the hips. As a result, clinicians may prioritize recommending an exercise program for patients with knee OA over patients with hip OA to treat their symptoms. However, results of the few studies assessing this topic were inconclusive.”
To address this knowledge gap, Dr. Roos and colleagues conducted a study, published in Osteoarthritis and Cartilage, comparing changes in outcome in patients with symptomatic knee or hip OA who took part in a longitudinal cohort study. “We utilized the large Good Life with osteoArthritis in Denmark (GLA:D) database in which outcomes are collected prospectively from patients with knee and hip OA treated with education and exercise therapy in primary care,” Dr. Roos says. “A total of 24,241 patients with knee OA and 8,358 patients with hip OA were included. Among the variables we compared between the groups were changes in pain intensity, knee injury/hip disability scores, QOL, and results of 40-meter walk tests at 3 and 12 months.”
Hip Vs Knee Osteoarthritis: Insignificant Differences in Outcome
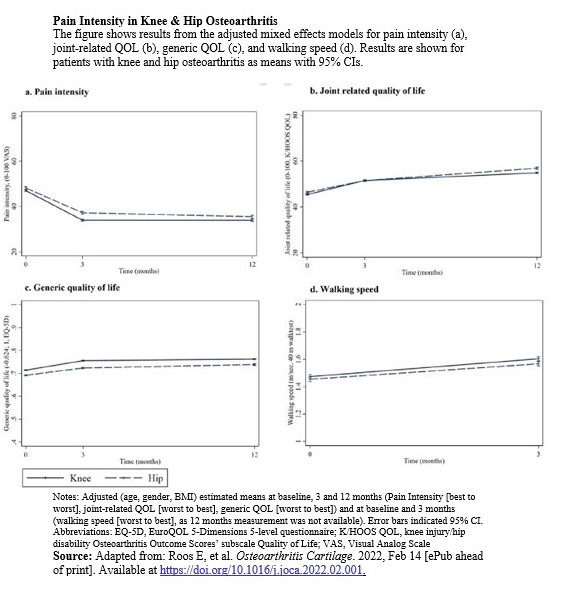
The common perception that patients with knee OA have better outcomes than patients with hip OA is incorrect, according to Dr. Roos and colleagues. “Patients with knee OA and hip OA were on average more alike in outcome than different,” Dr. Roos notes. “Symptom duration, pain intensity, use of pain medication, physical function, and QOL were similar in both groups. Over time, improvements were found in both groups and any differences in outcome between them were insignificant (Figure).”
The study team did observe more obesity among patients with knee OA than among those with hip OA. In addition, more patients with knee OA presented with bilateral symptoms. “We also found that symptoms in the hips of patients with knee OA were less common than symptoms in the knees of patients with hip OA,” Dr. Roos notes. “In patients with knee OA, previous injury and surgery were far more common than in those with hip OA.”
Don’t Prioritize Knee or Hip OA Over the Other
The study has some limitations, according to Dr. Roos, including the lack of a control group. “Therefore, the improvements we noted in patients cannot be credited entirely to the exercise program,” she says. “In addition, not all patients presented complete data or attended all follow-up visits.” However, these limitations affect patients with knee and hip OA alike and are unlikely to impact on the comparison.
The study team emphasizes that clinicians who work with patients with knee and hip OA should not prioritize one group over the other in regard to treatment. “We acknowledge that the treatment results are vastly similar for patients with knee and hip OA when undergoing patient education and supervised exercise therapy for 8 weeks,” adds Dr. Roos.
The researchers express the need for future research on the implementation of their findings in clinical practice. “We have sufficient data to know that exercise therapy works well for both groups of patients, and that exercise therapy is a cornerstone for the treatment of OA in all available clinical guidelines,” Dr. Roos says. “The mystery is why this treatment is not taken seriously or sufficiently implemented.”
 Physician's Weekly Admin
Physician's Weekly Admin
{kind=link}