

According to recent data, the suicide rate in the United States has risen by almost 30% over the past 2 decades, and healthcare settings can play a crucial role in identifying people who are at risk for suicide. “EDs may be particularly important for such efforts, but studies indicate that many ED patients have unrecognized suicidal risks because efforts tend to focus on managing their chief complaint,” says Edwin D. Boudreaux, PhD. Due to the busy nature of EDs, it can be challenging for ED clinicians to identify patients at risk for suicide.
Testing an Intervention
Recently, Dr. Boudreaux and colleagues conducted the ED Safety Assessment and Follow-Up Evaluation (ED-SAFE) as part of a multicenter collaborative study for quality improvement. The objectives of ED-SAFE were to develop and test a standardized approach to universal suicide risk screening within the general medical ED and to test an ED-initiated intervention with follow-up phone calls to reduce suicidal behaviors among people who screened positive for suicide risk. For a study published in the American Journal of Preventive Medicine, the research team reported their findings on the feasibility and impact of the screening protocols developed in ED-SAFE.
The investigation examined three separate phases in the study: 1) treatment as usual (Phase 1), 2) universal screening (Phase 2), and 3) universal screening plus the intervention (Phase 3). Data were included from eight participating EDs from seven different states from 2009 through 2014. “The screening protocol was brief, using three items,” explains Dr. Boudreaux. “It asked about depressive symptoms, active suicidal thinking, and lifetime suicide attempts.”
In Phase 1, patients were treated at all eight sites according to the site’s usual and customary practices. In Phase 2, universal suicide risk screening was implemented during routine care. In Phase 3, improvements were made to increase screening rates and fidelity. During all three phases, the research team carefully documented the proportion of patients who were being screened, and the proportion of those who were screened who were positive for suicidal thoughts or behaviors.
A Significant Impact
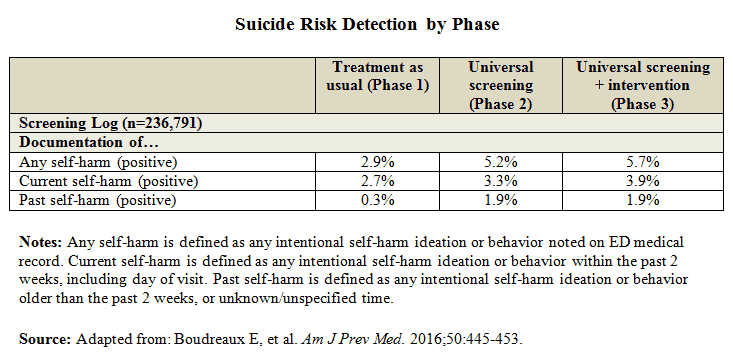
After reviewing more than 236,000 ED visit records across the three phases, the authors found that the rate of documents suicidal screenings increased from 26% in Phase 1 to 84% in Phase 3, representing an increase of more than 300%. This increase in screening led to a nearly two-fold increase in identification of patients positive for suicide risk. “Overall, detection rates rose from almost 3% before the intervention to nearly 6% after the intervention was implemented,” Dr. Boudreaux says (Table below). These trends in screening and detection persisted even after adjusting for factors such as site, demographics, and the quality of the screenings.
“Our research showed that we could improve suicide risk screening rates in the general adult ED population during routine care using simple protocols that could be tailored to the resources that were available at each ED,” Dr. Boudreaux says. The analysis also revealed that increasing screening for suicide led to nearly twice as many patients being identified as having suicidal risks, either by ideation or attempting to commit suicide. If the approach was used for the nearly 350,000 ED visits that occur each year at the eight EDs participating in the study, the authors noted that almost 10,000 additional ED patients with previously undetected suicide risks would be identified annually.
Considering the Implications
The study findings, if scaled beyond the ED-SAFE sites, have the potential to dramatically improve identification of nascent suicide risk in a highly vulnerable group, according to Dr. Boudreaux. “This data could possibly pave the way for applying interventions to reduce subsequent suicidal behaviors in a patient population that often has such risks go unaddressed,” he says.
Several important steps were taken to foster successful screening adoption, Dr. Boudreaux says. The research team developed a simple screening instrument and clinical protocols that were designed to be easily integrated into the ED routinely. Training was brief and available through multiple channels, including in-person modules that were conducted by a site trainer or online. The eight EDs participating in the study also used widely available performance improvement methodologies, including “plan–do–check–act” cycles, for integrating the protocols into routine care and monitoring performance.
“These steps are critical to ensuring positive outcomes with the intervention, but it’s important to be flexible with protocols and make sure that screenings are conducted the right way,” says Dr. Boudreaux. “The next step is for EDs to work on strategies to ensure that patients who screen positive for suicidal thoughts are managed accordingly. If we can find ways to optimize linkage to care for positive screeners, we have a real opportunity to reduce the burden of suicide in the U.S.”
Edwin D. Boudreaux, PhD, has indicated to Physician’s Weekly that he has or has had no financial interests to report.
 PhysWeekly
PhysWeekly