

National estimates show that nearly 500,000 Americans seek medical treatment for burn injuries each year. Burn centers have the infrastructure, personnel, and resources to appropriately care for individuals who sustain these injuries, but many patients are initially triaged at centers without burn capabilities. Delaying the transfer of patients with burn injuries to facilities with burn-specific capabilities can potentially increase risks for adverse outcomes.
Decisions on whether to transfer patients to a burn center depend on the extent and type of injury. The American Burn Association has developed criteria as a triage tool to guide decision making on transferring burn patients to specialized centers, but these criteria are not strict guidelines. “Transfers between hospitals can take several hours, which can result in worsening of the patient’s condition, lapses in care, and delays in treatment,” says Matthew C. Bozeman, MD. Unwarranted transfers, he adds, may lead to inefficient use of important healthcare resources while also increasing costs and unnecessarily inconveniencing patients.
Severe Burn Injury Cases More Likely to Be Transferred to Burn Centers
For a study published in the Journal of Burn Care & Research, Dr. Bozeman and colleagues assessed how transfer-associated treatment delays affected outcomes among 122 patients treated for burns. Investigators retrospectively identified adult burn patients who met the American Burn Association criteria for being transferred. Patients were evenly divided into two cohorts, with one group including individuals who were directly admitted to a burn center from the field while the other cohort included patients who were transferred to a burn center from an outlying facility.
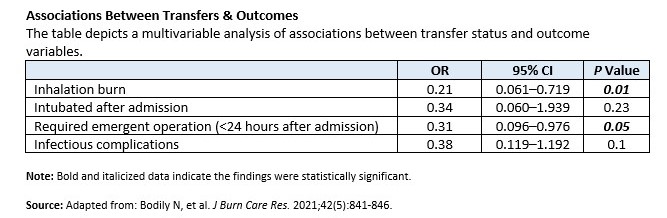
According to the results, transfer patients experienced a longer median time from injury to burn center admission than those who were directly admitted to a burn center. “Patients who were directly admitted to burn centers were more likely to have inhalation burns, need intubation after admission, require an emergent procedure, and develop infectious complications,” says Dr. Bozeman. No major differences were seen between groups with respect to ventilator days, total number of operations, total length of stay, disposition, or mortality. In a multivariable analysis that controlled for age, concomitant injuries, and percentage of total body surface area burned, the greater frequency of inhalational injury and emergent procedures for directly admitted patients remained significant (Table).
Findings from the study suggest that patients with more severe, higher acuity injuries were more likely to be immediately identified and taken directly to a burn center, according to Dr. Bozeman. For patients with less severe, lower acuity injuries who otherwise met the American Burn Association criteria to be transferred to a burn center, researchers found that short delays in being transferred did not affect patient outcomes overall.
Significant Implications Regarding Cost & Resource Utilization
Implications of the study are significant in terms of cost and resource utilization, according to the study authors. Patients with significant burn injuries and/or compromised airways were more likely to be promptly identified and taken directly to a burn center, Dr. Bozeman says. “However, initially triaging patients with lower acuity burns at an outlying facility may present an opportunity to avoid unnecessary transfers,” he says. “This may decrease costs and resource utilization without harming patients.” Improving how burn injuries are assessed at outlying facilities may prevent unnecessary transfers of patients and the associated transfer costs for individuals who might otherwise be adequately cared for at a facility without specialized burn care.
The study team notes that it is expanding on its findings by developing a burn referral line, which will be available for use by critical access centers at all hours. The initiative will include video evaluations of burn injuries by an on-call provider at a burn center facility. Dr. Bozeman adds that the team developed telemedicine burn care courses for first responders and referring centers. Additionally, the researchers have successfully transitioned half of their burn clinic follow-up visits to telemedicine, which may be particularly beneficial when managing patients who live in more remote areas.
 Martta Kelly
Martta Kelly
{kind=link}