

Recent estimates show that urinary tract infections (UTIs) are among the most common bacterial infections occurring in the United States. There are more than 8 million annual office visits and 1 million ED visits for UTIs annually, with about 100,000 cases resulting in hospitalizations. “UTIs are twice as common among women of all ages when compared with men,” says Lona Mody, MD, MSc. “Asymptomatic bacteriuria, urinary incontinence, and symptomatic UTIs are especially prevalent in older women, but it can be difficult for clinicians to identify which patients warrant antibiotic therapy.”
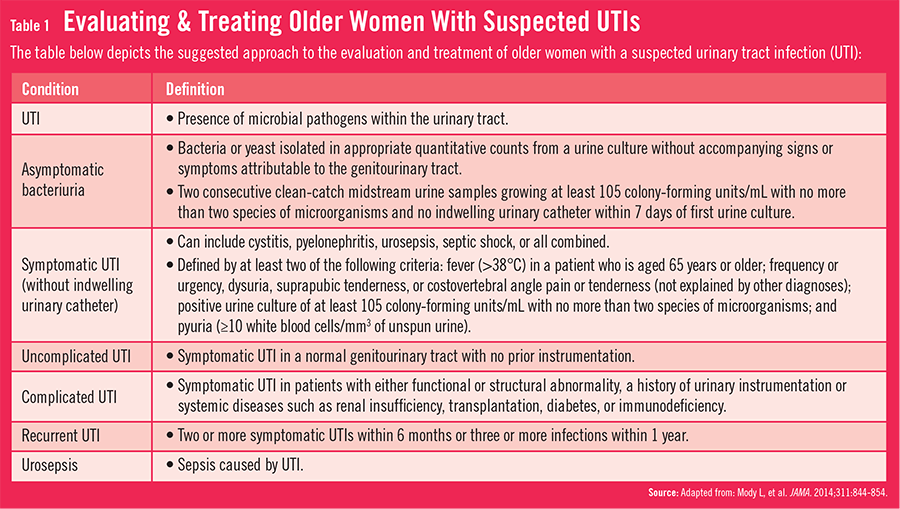
In an issue of JAMA, Dr. Mody and Manisha Juthani-Mehta, MD, had a clinical review published in which the authors looked at the management of asymptomatic bacteriuria and symptomatic UTIs among older community-dwelling women. The spectrum of urinary conditions can range from asymptomatic bacteriuria to symptomatic UTIs or worse (Table 1). “Many symptoms of UTIs mimic other problems that can affect older women,” explains Dr. Mody. “This can make it challenging for clinicians to know when and how to treat patients.”
{kind=link}
Making a Diagnosis
The review article by Dr. Mody and Dr. Juthani-Mehta notes that asymptomatic bacteriuria is generally benign in older women. However, the diagnosis of a symptomatic UTI can be more challenging when considered in the context of chronic genitourinary symptoms, increasing cognitive impairment, and comorbidities from advancing age. When evaluating new dysuria, several factors are important, including timing, severity, and location. Worsening urinary frequency or urgency can occur for both UTIs and in urinary incontinence, making these symptoms unreliable indicators for UTIs. Conversely, new dysuria is more specific for symptomatic UTIs. If this is present, there is a need for further diagnostic evaluation.

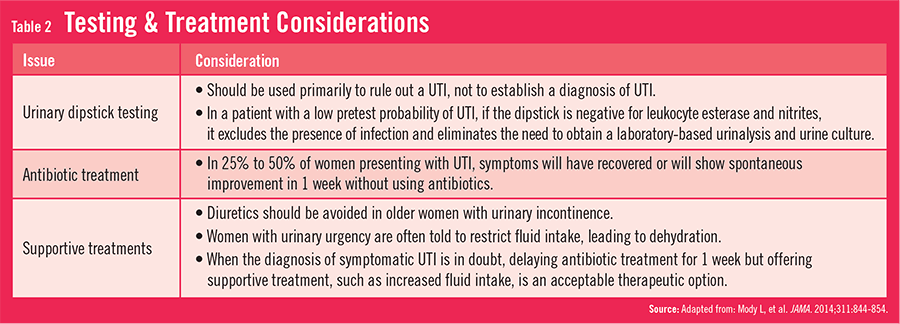
“Establishing a diagnosis of symptomatic UTI in older women will often require assessing patients for new presenting signs and symptoms of genitourinary tract disease and considering other diagnoses,” Dr. Mody says. “Clinicians need to be careful with their assessments and consider using urinalysis and urine culture. It’s important to get confirmation from laboratory results.” She says that clinicians should take into account several factors when deciding on testing and treatment options for UTIs in older women (Table 2). In older patients with a high prevalence of genitourinary symptoms, urinary studies should only be conducted if symptoms worsen acutely and there is no other identifiable cause. Non-specific symptoms should not be the only reason for obtaining urinary studies.
{kind=link}
Hydration is another often unrecognized factor to consider when managing older women with suspected UTIs, according to Dr. Mody. “Many women with suspected UTIs are thought to have urinary urgency,” she says. “If so, they are likely to be told to restrict fluid intake, which can lead to dehydration. Unfortunately, this can play a role in the development of UTIs. When a diagnosis of symptomatic UTI is in doubt, it may make sense to delay antibiotic treatment while conducting further evaluations. However, supportive treatments, such as hydration, should be offered.”
Treatment Considerations
Once a diagnosis of symptomatic UTI is made, antibiotics should be chosen based on prior uropathogen susceptibility profiles. “Clinicians should consider the possible adverse effects of giving antibiotics to older women for UTIs,” says Dr. Mody. “We should think about potential interactions with other medications and other comorbidities that patients may have. In some cases, it may be more beneficial for patients to wait a week before prescribing an antibiotic because symptoms can dissipate.” She notes that the choice of antibiotic and duration of therapy are two important issues that require consideration when treating older patients for UTIs.
Prevention Efforts
To prevent UTIs from occurring in the future, Dr. Mody and Dr. Juthani-Mehta recommend taking time to educate women about the efforts they can take to avoid UTIs. For example, recent studies on postmenopausal women suggest that sexual intercourse can increase the risk of symptomatic UTIs. Clinicians should discuss safe sex practices with their patients. The dialogue may also include a conversation about using cranberry products and prevention strategies. Before initiating any prevention strategy, medications that may contribute to urinary retention should be evaluated. In addition, urologic evaluations are recommended for those who may have predisposing conditions to UTIs, such as pelvic organ prolapse, bladder lesions, or kidney stones.
“More research is needed on the prevalence of both asymptomatic and symptomatic UTIs,” says Dr. Mody. “In addition, we need studies that help determine if we can avoid using antibiotics in these older adults by better differentiating asymptomatic bacteriuria from more serious and symptomatic UTIs. As this information emerges, clinicians will hopefully be able to better diagnose and treat UTIs in older women in the future.”