

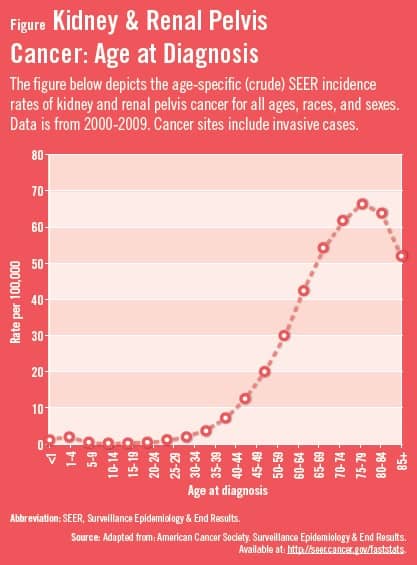
Data from the American Cancer Society estimate that 65,150 new cases of kidney cancer, including renal cell carcinoma (RCC), renal pelvis carcinoma, and Wilms tumor, are expected to be diagnosed in the United States in 2013.1 Kidney cancer is among the 10 most common cancers in both men and women. Approximately 90% of renal tumors are RCC, and 85% of these are clear cell tumors.2 From 2005 to 2009, kidney cancer incidence rates increased by 3.1% per year, primarily because of an increase in the detection of early stage disease. Most people with kidney and renal pelvis cancer are older when they are diagnosed (Figure),3 with the median age at diagnosis being about 65.2
An estimated 13,680 deaths from kidney cancer are expected to occur in 2013. Overall, the mortality rate for kidney cancer decreased by an average of 0.5% per year from 2005 to 2009.1
Recent estimates suggest that 20% to 30% of RCC patients present with metastatic disease.4 About 70% of RCC patients develop metastases during the course of their disease. The 5-year survival rate for patients with metastatic RCC (mRCC) is 11.6%, which is significantly lower than that of localized or regional RCC (Table).2
Treatment
According to Robert A. Figlin, MD, FACP, interleukin-2 (IL-2) was the previous standard of care for mRCC in the 1990s. “While response rates were low, about half of mRCC patients who responded to IL-2 demonstrated long-term disease-free survival, and some of these patients were completely cured. However, the side effects associated with IL-2 were severe.”
As clinician researchers have gained an improved understanding of the biology of kidney cancer, several targeted therapies have been developed that inhibit cancer growth.1 “In mRCC, oral therapy has recently emerged as the standard of care for the overwhelming majority of patients,” Dr. Figlin says. “Oral therapy can benefit mRCC patients who develop metastatic disease following primary tumor resection, or for those who present with metastatic disease. When choosing an oral therapy, clinicians should examine the evidence associated with an agent. Oral therapies being considered should have a high level of efficacy in published clinical trials. Tolerability is also important because each agent has a different toxicity profile, adverse reactions (ARs), and side effects.”5
Goals of Oral Therapy
According to Dr. Figlin, duration of oral therapy is critical. “When possible, the goal should be to maintain the full starting dose for the duration of treatment so that outcomes may be optimized,” he says. “Historically, the dose of intravenous cancer therapies could be modified to ameliorate side effects. The oral therapy era is different in that clinicians must now find ways to help ameliorate some side effects while maintaining the optimal drug dosage. 6 For clinicians, when possible, the goals are to start oral therapy at full dose, maintain the full dose, and be proactive about managing toxicity in order to maintain the full dose.”
Maintenance of Oral Therapy
Oral therapies are powerful medications, which have been shown to have serious potentially life-threatening side effects, in addition to low-grade ARs. Dr. Figlin says clinicians should aggressively address toxicities as early as possible, especially low-grade ARs. “As toxicities become cumulative, they are more difficult to treat. While low-grade ARs are rarely life-threatening, they have the potential to be life-altering.”
Using a multidisciplinary team approach is recommended when treating mRCC with oral therapy. “With oral therapy, a team approach should involve other specialists in patient care, especially oncologic nurses,” Dr. Figlin says. “Many of the low-grade ARs that occur with oral therapy can be handled on an outpatient basis—over the phone by a nurse, for example—rather than during office or hospital visits. Oftentimes, a simple discussion can be the most effective strategy to help ensure that patients do not develop cumulative toxicities. Involving physicians outside of oncologists may also be necessary, depending on the clinical makeup and comorbidities of patients.”7
When using oral therapy, if possible, clinicians and other members of the multidisciplinary team should develop strategies to aggressively manage ARs, should they occur. Some ARs may be unmanageable and require discontinuation of therapy. “Informing patients on what to do if toxicities occur can help reduce the risk of cumulative toxicities occurring,” says Dr. Figlin. “Clinicians should understand the information in package inserts of oral therapies and stay abreast of the literature. This will assist clinicians as oral therapies are selected for patients. It will also enhance our ability to be proactive and to help ensure that patients maximize their chances of staying on the full dose for the duration of use.”
 admin
admin
{kind=link}
{kind=link}