

Despite advances in multiple myeloma (MM) treatment, research suggests that survival outcomes can vary depending on factors that may be related to the tumor, the host, or both. “Different prognostic systems have been developed using one or more of these factors to better predict outcomes in patients with MM,” says Shaji Kumar, MD. These include the International Staging System (ISS) and its successor, the revised ISS (R-ISS), and the International Myeloma Working Group risk stratification.
Studies suggest that the presence of various genetic abnormalities appears to be the strongest driver of outcomes among patients with MM. “Given that patients with high-risk MM have survival that is nearly one-third of what is seen among those without high-risk abnormalities, the ability to better predict the outcomes is important to determine the patient’s prognosis,” Dr. Kumar says. “The R-ISS includes serum albumin, beta-2 microglobulin, LDH, and high-risk cytogenetic markers. While the R-ISS is a powerful prognostic tool, it leaves out important high-risk genetic markers and does not distinguish patients with multiple genetic abnormalities from those with a singular high-risk abnormality.”
The Mayo Additive Staging System for Newly Diagnosed Multiple Myeloma
For a study published in Blood Cancer Journal, Dr. Kumar and colleagues evaluated a new simple additive staging system called the Mayo Additive Staging System (MASS) in patients with newly diagnosed MM. The authors developed and validated MASS, which incorporates additional fluorescence in-situ hybridization (FISH) abnormalities not included in the R-ISS. The researchers first evaluated the prognostic value of predefined cytogenetic and laboratory abnormalities in 2,556 patients diagnosed with MM between 2004 and 2019. They then used data from 1,327 patients to develop a risk stratification model, which was then validated in 502 patients.
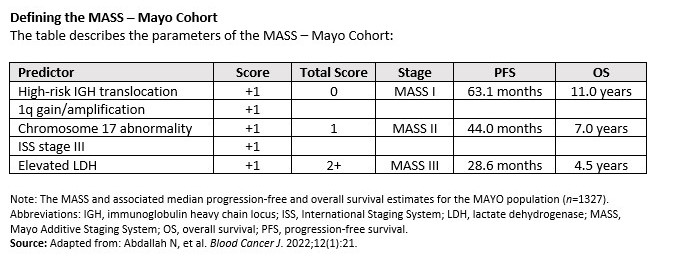
The additive staging system assigned similar prognostic values to a set of five prognostic variables that were shown to be the most impactful. “These variables included ISS stage III, elevated serum LDH, deletion 17p, chromosome 1q gains or amplification, and the presence of high-risk translocations involving chromosome 14,” Dr. Kumar explains. “By grouping patients into those with no risk factors, one risk factor, and two or more risk factors, we identified three populations with very different survival outcomes.”
Overall survival (OS) was 11.0 years in newly diagnosed patients with no high-risk factors, compared with 7.0 years in those with one high-risk factor and 4.5 years in those with two or more high-risk factors (Table).
The prognostic utility of the additive staging system was demonstrated in older and younger patients, and its prognostic utility was shown in transplant-eligible and ineligible patients, during two periods, and in two independent populations. “Our simplified system offers more granularity to prognostication and provides a framework for designing clinical trials targeting high-risk disease,” notes Dr. Kumar. “Our study is also one of the largest to look at all the different risk factors that have been described and are easily available in clinical practice.”
Identifying Subgroups With Multiple Myeloma at Risk for Poor Outcomes
The five commonly available laboratory variables utilized in the study can provide a good estimate of survival outcomes based on current therapies, Dr. Kumar says. “Our findings highlight the need to conduct baseline cytogenetic assessments in all patients with newly diagnosed MM using FISH,” he says. “We also demonstrated that this risk stratification system is easily applicable across the newly diagnosed MM patient population. Furthermore, we found that increasing numbers of risk factors continue to worsen the prognosis of patients. These data can enable us to identify subgroups of patients that are likely to experience poor outcomes.”
Dr. Kumar says the current system provides a basic framework in which other high-risk characteristics can be added as they become validated. “As we learn more, risk stratification systems will continue to evolve,” he says. “A better understanding of the disease biology that drives poor outcomes—which is likely to vary from patient to patient—will allow us to develop therapies that can be targeted more specifically toward the underlying biology. This may take the form of targeted drugs that can be added to current treatment mainstays.”
 Martta Kelly
Martta Kelly
{kind=link}