

For patients with burn injuries who received a CT scan with IV contrast, there was no increased risk for AKI, even among those with significant burns.
Acute kidney injury (AKI) can have a significant impact on morbidity and mortality in patients who suffer burn injuries. “AKI is a serious and very common complication in patients with burn injuries,” says Jessica R. Burgess, MD, FACS. “Unfortunately, patients with burn injuries may have also suffered blunt trauma if their burn was the result of an explosion, car fire, jumping from a burning building, or a similar such event.” Several risk factors for developing AKI in patients with burn injuries have been identified, including age, total body surface area (TBSA), and high baseline serum creatinine and blood urea nitrogen.
Patient sedation, difficulty performing physical exams because of the extent of burn injuries, and full thickness burns can hinder the accurate identification of underlying injuries in trauma patients with severe burns. “It’s important to obtain CT imaging as part of the patient’s initial workup to rule out other trauma,” explains Dr. Burgess. “However, physicians may be hesitant to obtain a CT with intravenous (IV) contrast media (CM) in patients with burn injuries due to concerns that they may develop an AKI secondary to their injury or contrast-induced nephropathy (CIN).” CIN is a potentially serious complication of using IV CM during imaging procedures.
Multicenter Retrospective Chart Review Conducted in Level I Trauma Centers
For a study published in the Journal of Burn Care & Research, Dr. Burgess and colleagues explored if patients with burn injuries undergoing initial CT imaging with IV CM on admission had a higher incidence of AKI when compared with those who did not undergo imaging. Between 2014 and 2017, the researchers conducted a multicenter retrospective chart review of patients admitted to two level I trauma centers with TBSA burns of 10% or more. The study included 439 patients, 67 of whom underwent CT scans with IV contrast on admission.
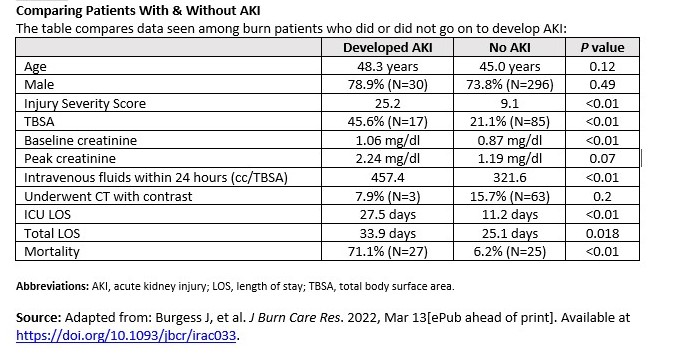
According to the results, 8.4% of all patients in the study developed AKI. The rate of AKI between patients who received a CT scan was 9.1%, compared with 6.0% for those who did not receive CT scans, but this finding was not statistically significant. When compared with patients who did not develop an AKI, those who developed an AKI were more likely to have a higher TBSA, higher Injury Severity Scores, longer lengths of stay, and higher mortality (Table).
Intravenous CM Does Not Increase Risks for AKI in Patients With Burns
“Our most important finding was that for patients with burn injuries who received a CT scan with IV contrast, there was no increased risk for AKI, even among those with significant burns,” Dr. Burgess says. Although patients who underwent CT were sicker, it did not result in a significant increase in AKI or mortality. In additional subgroup analyses of patients whose TBSA was 40% or higher, no association was seen between administering IV CM and developing an AKI. “Ultimately, the size of the burn was the greatest predictor of the development of an AKI,” says Dr. Burgess.
Hesitation to use imaging on burn patients because of concerns about an AKI or CIN may impact clinical decision making, Dr. Burgess points out. Thorough imaging is needed to avoid missed opportunities to identify potentially life-threatening underlying injuries. Selective-CT scanning should not be favored over whole-body CT scanning in these patients. “Based on the results of our study, it’s safe to obtain a CT scan with IV CM in trauma patients with burns and should not be avoided out of concern for CIN,” says Dr. Burgess.
Mitigation Strategies Are Key for Decreasing Morbidity
The study group recommends all patients with burn injuries with concomitant blunt trauma and who are suspected of having underlying injuries undergo appropriate and complete imaging with IV CM. With this approach, clinicians can be confident they are not contributing significantly to their patients’ risk for AKI. This can empower clinicians to help their patients avoid the potentially devastating consequences of missing an underlying injury.
“Emerging research into possible mitigation strategies will play an important role in decreasing the morbidity associated with these injuries,” Dr. Burgess says. “Trauma patients also may require multiple doses of contrast for their injuries. In addition, it would be meaningful to clinicians if future studies further examine the actual risk for AKI in these patients.”
 Martta Kelly
Martta Kelly
{kind=link}