
“Childhood food allergy (FA) is steadily increasing globally and represents a serious public health problem for the 3% to 8% children affected,” explains Antonella Muraro, MD, PhD. “FA is also the first cause of anaphylaxis in children, with a seven-fold increase observed from 1992 to 2012. The current standard of care is allergen avoidance and prompt treatment of allergic reactions with adrenaline auto-injectors. However, accidental reactions are common: 72% of preschoolers had a FA reaction during a period of 36 months; 53% experienced more than one. In addition, more than 25% of the first reactions occur in the community, at school, in the cafeteria, or in a restaurant where emergency facilities are lacking. A constant fear of allergic reaction, the need to carry adrenaline auto-injectors everywhere, and the task of checking food labels hugely impacts a patient’s, and caregiver’s, QOL.”
There is increasing interest in allergen-specific immunotherapy and biologic treatment, Dr. Muraro points out, but there are inconsistent results; some studies demonstrate improved allergen tolerance, while others underscore higher rates of adverse reactions. “After gathering feedback from people with FA, patient advocates, healthcare professionals, teachers, and policy makers, we prioritized two key questions,” she says. “What is the efficacy, safety, and cost-effectiveness of immunotherapy alone, immunotherapy with a biologic, or biologics alone for children and adults with any IgE-mediated FA compared to no active treatment agent? Also, what is the efficacy, safety, and cost-effectiveness of immunotherapy administered by different routes for children and adults with any IgE-mediated FA?”
Oral Immunotherapy Increased Patient Tolerance
For a paper published in Allergy, European Journal of Allergy and Clinical Immunology, Dr. Muraro and colleagues sought answers to these questions by searching six databases for randomized controlled trials (RCTs) about immunotherapy alone or with biologics (to April 2021) or biologic monotherapy (to September 2021) in FA. The researchers pooled the data and included 36 trials about immunotherapy with 2,126 participants, most of whom children.
“We found that oral immunotherapy increased patient tolerance while on therapy for peanut, cow’s milk, and hen’s egg allergies,” Dr. Muraro notes. Oral immunotherapy did not lead to heightened adverse reactions or severe reactions in peanut allergy but could increase mild adverse reactions in cow’s milk and hen’s egg allergy. Epicutaneous immunotherapy improved patient tolerance while on therapy for peanut allergy.
Adverse Reactions Were Mild to Moderate
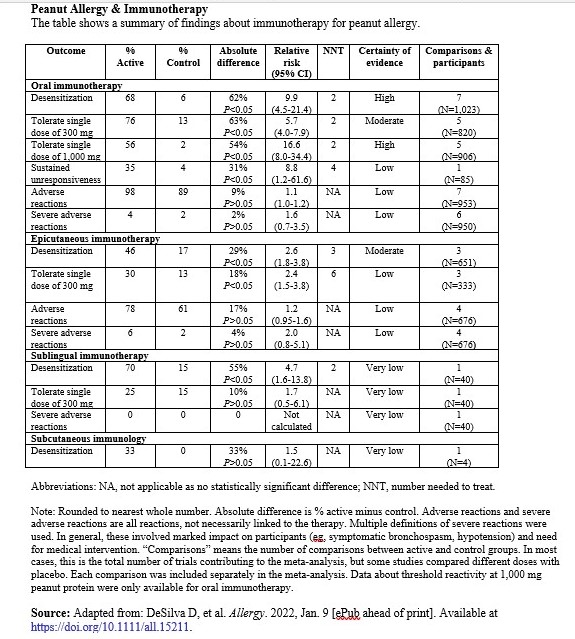
“Oral immunotherapy and epicutaneous immunotherapy appear safe and effective in achieving desensitization, mainly in children,” she says, adding that the treatment resulted in a large increase in the proportion of people able to tolerate peanut. Those receiving oral immunotherapy were six times more likely than controls to tolerate a single dose of 300 mg (roughly one peanut), and 17 times more likely to tolerate 1,000 mg. Prior to immunotherapy, the mean maximum tolerated dose was only about 34 mg. Those receiving epicutaneous immunotherapy were twice as likely as controls to be able to tolerate a single peanut dose of 300 mg. Adverse effects were mostly mild to moderate and even the few severe reactions were able to be properly managed without any fatalities (Table).
“The latest robust evidence supports more proactive management strategies such as the use of some types of allergen-specific immunotherapy for selected children with IgE-mediated FA,” Dr. Muraro says. “Today’s physicians, allergists, and immunologists have an opportunity to offer an effective treatment, besides the avoidance diet, to increase the threshold of reactivity in cow’s milk, egg, and peanut allergy, reducing the risk for unexpected severe reactions. The selection of patients for FA immunotherapy should be done with great care, where patients’ characteristics, physicians’ expertise, and facilities are adequately considered in a cost-benefit assessment.”
Dr. Muraro and colleagues concur that further research should focus on several areas. “Biomarkers should be developed to evaluate the risk for reactions and probability to achieve tolerance when the treatment is suspended. This would allow clinicians to tailor the right FA immunotherapy to the right patient and to maximize QOL. The role of biologics alone, or in combination with FA immunotherapy, appears very promising but should be better investigated through RCTs. In addition, QOL and cost effectiveness need to be studied to ensure access to the treatment and prevent inequalities. We are just at the beginning of an exciting journey to find a cure for FA.”
 Martta Kelly
Martta Kelly
{kind=link}