
Multiple myeloma (MM) is always preceded by a precursor condition called monoclonal gammopathy of undetermined significance and sometimes by an intermediate stage referred to as smoldering MM (SMM). Therefore, it is extremely important for clinicians to make an accurate diagnosis of MM, which requires therapy, versus a precursor state that needs to be observed without therapeutic intervention.
The diagnostic criteria for MM were revised in 2014 to include those individuals with clinical or laboratory characteristics that predict a high risk for progression to active myeloma from the precursor state of SMM in a relatively short time frame. One of the criteria included was a free light chain ratio (FLCr) of ≥100. Typically, the excess FLC (Kappa or Lambda) that is secreted by the monoclonal plasma cells would spill into the urine where it could be detected and measured in a 24-hour urine sample. The level of elevation in FLC that would meet the criteria for diagnosis of active MM is typically associated with measurable levels of light chain in the urine as well.
Subgroup of Patients With Elevated FLC Levels With Insignificant Light Chain in Urine
However, we have observed a subgroup of patients who may have significantly elevated FLC levels in the serum without significant amounts of light chain in the urine. We believe that this may be related to dimerization or polymerization of the light chains that prevents it from being spilled into the urine. In this scenario, it is likely that the level of FLC in the serum is artificially high and may not carry the same risk for disease progression.
Therefore, we hypothesized that patients with high levels of serum FLC without any significant measurable amount of monoclonal protein in the urine will not have the same risk for progression as those patients with high serum FLC levels and measurable urine monoclonal protein (uMCP). For a research letter published in Leukemia, my colleagues and I sought to test our hypothesis. We examined a well-defined cohort of patients with MM (N=822) who have been observed at our institution and followed up over time.
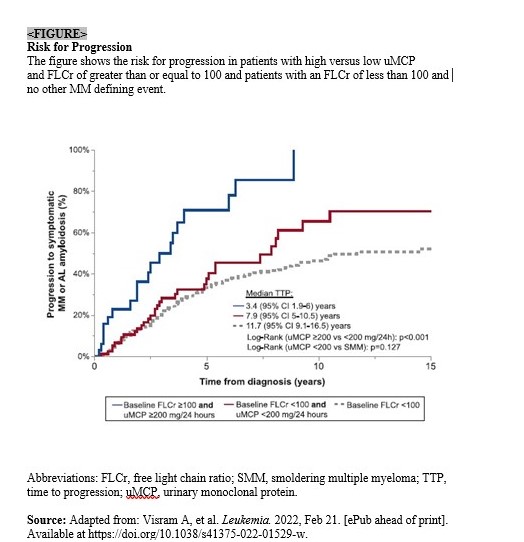
We investigated the laboratory parameters associated with risk for progression to active MM. The endpoint was development of active myeloma that required therapy. Patients were divided into three groups: 1) those with a FLCr of greater than or equal to 100 with at least 200 milligrams of an M protein spike in the urine, 2) those with a FLCr of greater than or equal to 100 with less than 200 milligrams of an M protein spike in the urine, and 3) those with a FLCr of less than 100. We then examined the risk for progression to active myeloma within the context of other known risk factors for progression.
We found that the risk for disease progression was significantly higher among patients with greater than or equal to 200 versus less than 200 mg/24-hour uMCP excretion in the presence of a serum FLCr of greater than 100. In addition, patients with a low uMCP excretion had a similar risk for progression to symptomatic MM/light chain amyloidosis compared with patients with SMM with a baseline FLCr of less than 100.
24-Hour Urine Protein Electrophoresis Is Crucial
Our findings emphasize the importance of performing a 24-hour urine protein electrophoresis to ensure there is a measurable M spike in the urine before one applies the criteria of serum FLCr of greater than or equal to 100 for diagnosing a patient with active MM. Patients who do not excrete much light chain in their urine have a low risk for progression to myeloma, which in many of these patients means development of renal insufficiency. These patients should be monitored for other markers that may increase the risk of progression (Figure).
For future research, my colleagues and I would like to continue to identify risk factors that increase the risk for progression from precursor stages to active myeloma. Our goal is to identify those patients with a high risk for progression so that treatments can be started earlier. This will also allow us to examine prevention strategies in patients with a high risk for progression but who do not meet the criteria for active myeloma, the group of patients whom we currently define as “high risk smoldering myeloma.”
 Martta Kelly
Martta Kelly
{kind=link}