
“HF is a very common condition, with HF exacerbations accounting for a large number of ED visits and hospitalizations,” Maliha Zahid, MD, PhD, notes. “Twenty years ago, HF with preserved ejection fraction (HFpEF) accounted for approximately 30% of all cases of HF. That percent has risen to slightly more than 50%. With the aging of the population, this fraction is expected to only increase with time. Hence, looking at predictors of mortality in HFpEF specifically can help clinicians stratify risk and better plan patient care.”
For a paper published in The American Journal of Cardiology, Dr. Zahid and colleagues conducted an observational study of patients with a primary diagnosis of congestive HF at the time of discharge from one of three hospitals in a community health system. “We set out to study a real-world HFpEF patient population with left ventricular ejection fraction greater than 50% that presented with a primary, physician-determined diagnosis of HF exacerbation,” Dr. Zahid says. “This allowed us a median follow-up of 28 months during which we could observe all-cause mortality and do meaningful survival analyses to see which factors contributed to this outcome.”
The study was conducted from January 2014 to January 2017. Researchers obtained data on demographics, lab results, and echocardiograms performed closest to the index hospitalization from 487 patients with a mean age of 80.5, almost all of whom were White (98.8%).
Several Characteristics for All-Cause Mortality Identified
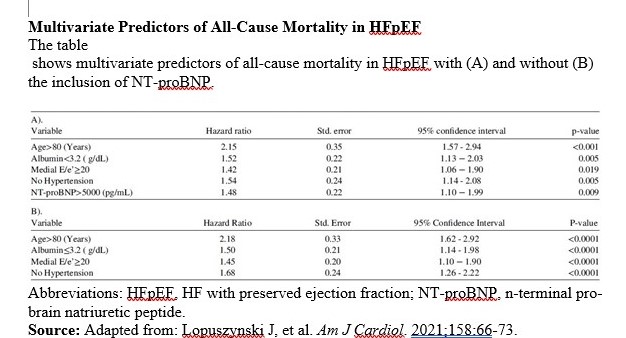
Dr. Zahid and colleagues identified several characteristics that were predictive of all-cause mortality in HFpEF, including age (>80), albumin (<3.2 g/dL), mitral medial E/e’ ratio (≥20), N-terminal pro-brain natriuretic peptide (NT-proBNP; >5,000 pg/mL), and no diagnosis of hypertension.
“In addition to lack of hypertension, low albumin and extreme old age were important prognosticators,” Dr. Zahid notes. “At the same time, nearly all patients had elevated NT-proBNP levels. Echocardiographic presence or call of diastolic dysfunction was not helpful prognosticators, but an elevated medial E/e’ ratio of greater than 20 was predictive.”
The incidence of all five of these variables resulted in a mortality rate of 72%, according to Dr. Zahid. Even when excluding NT-proBNP, the incidence of the other four factors was still associated with a mortality rate of 70%. “The presence of these factors is additive in nature,” she says. “If all four are present, a case for end-of-life planning, depending on patient/family preference, is one option.”
Absence of Hypertension as Poor Prognosticator Surprising
The researchers note that the absence of hypertension as a poor prognosticator was surprising (Table). “Uncontrolled, long-term hypertension is a pathophysiological mechanism leading to HFpEF, “Dr. Zahid says. “However, other studies have pointed out that decreasing blood pressure, or patients being steadily taken off their anti-hypertensives in old age, is an ominous finding. This could represent a ‘burnt-out’ stage of HFpEF, indicating a high probability of short- or intermediate-term mortality in the ensuing 2-3 years.”
However, the researchers believe the prognosticators they did identify can assist clinicians who treat HFpEF, which is challenging, according to Dr. Zahid. “Unlike HF with reduced ejection fraction, we really do not have much to offer patients other than symptomatic control, and perhaps sodium-glucose cotransporter-2 inhibitors that have modest benefit in reducing HF hospitalizations in patients with ejection fractions of 40% to 50%,” she notes. “I hope my colleagues can use the identified prognosticators to help their patients suffering from this recalcitrant disease by matching therapeutic intensities with disease stage. The findings may even help patients navigate end-of-life decisions.”
Dr. Zahid also hopes future studies include a more diverse patient population. “One major limitation of our study is that our patient population is predominantly White, though this did reflect the local patient population served by the community health system,” she says. “Women represented nearly two-thirds of the population, but mortality rates were similar between men and women. We cannot extrapolate our findings to Black, Hispanic, or Asian communities. Further studies of patients in more ethnically diverse populations are needed before these findings can be applied to non-White patients.”
 Physician's Weekly Admin
Physician's Weekly Admin
{kind=link}