

The costs associated with hospital readmission within 30 days of discharge are high. CMS and other payers are now measuring readmission rates and penalizing hospitals financially for poor performance. As a result, reducing readmissions has become a high priority in hospitals throughout the United States. In August 2012, my colleagues and I released a white paper on the current status of work to reduce readmissions and assess the problem in the larger context of accountable care.
Promising Approaches to Hospital Discharge
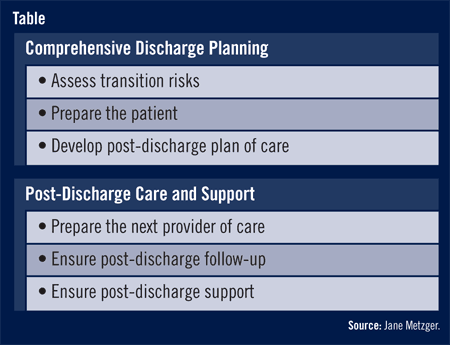
Thanks to a decade of experience in leading hospitals and considerable research, the important elements of discharge planning and post-discharge care and support have been identified (Table). But there are many ways to accomplish each element. No “magic bullet” set of interventions exists for every patient because individual risk factors do not triage patients for specific interventions, many possible care breakdowns can also contribute, and some factors are outside the control of the hospital.
Most hospitals routinely discharge all patients with an appointment for follow-up care and provide telephone outreach within a day or two to answer questions and check on status. The intensity of additional services and outreach is gauged to patient- and situation-specific risks to recovery and a smooth transition to the next provider of care.
Health Information Technology
Three key processes highly reliant on health information technology (HIT) are 1) medication reconciliation, 2) communication of patient status and discharge plans of care to receiving providers, and 3) tracking patients after discharge to ensure that care and support is received. HIT is necessary to record and communicate information and close potential loose ends. With greater adoption of HIT, providers will have access to more complete patient information and standards for communicating with clinical partners via health information exchange. As health systems leverage these to integrate HIT across sites and settings of care, they are building critical information links for continuity of care.
Accountable Care
Accountable care is already beginning to take hold throughout the U.S. Groups of providers are assuming responsibility across the continuum of care under reimbursement contracts that carry strong incentives to perform well on quality indicators and reduce spending growth. One of the biggest challenges will be overcoming fragmentation of care with new processes that proactively coordinate transitions, such as a hospital discharge. The collaboration, the processes, and the HIT infrastructure for addressing readmissions are great learning grounds for care coordination applied more broadly.
| Download the Whitepaper for Free!
For access to the full whitepaper titled “Preventing Hospital Readmissions: The First Test Case for Continuity of Care” by Metzger and colleagues, go to http://assets1.csc.com/health_services/downloads/CSC_Preventing_Hospital_Readmission.pdf. |
 TimH
TimH
{kind=link}