

New research was presented at SCCM 2015, the Annual Congress of the Society of Critical Care Medicine, from January 17 to 23 in Phoenix. The features below highlight some of the studies emerging from the conference that are relevant to emergency physicians.
Advanced Directives & Intubated ED Non-Survivors
The Particulars: Studies have shown that patients who are intubated in the ED have a high in-hospital mortality rate. However, little is known about the impact of advance directives on mortality.
Data Breakdown: Patients intubated in the ED who died before hospital discharge were reviewed in a study to calculate the proportion of those who received at least one code, had a do not resuscitate (DNR) order, and/or had care withdrawn. Within 48 hours of admission, 72% of patients had died, 40% had received at least one code, and 59% ultimately had care withdrawn. A DNR order was placed during the hospital course for 17% of patients.
Take Home Pearl: The majority of patients intubated in the ED who do not survive appear to die within 48 hours, and many ultimately have care withdrawn.
A Look at ED Visits Attributed to Rape
The Particulars: In the United States, data are lacking on the impact of rape on medical care and outcomes. Nationally representative epidemiologic estimates of ED visits attributed to rape may shed some light on this research gap.
Data Breakdown: For a study, researchers analyzed all ED visits with an external cause of injury code for rape using the Nationwide Emergency Department Sample. Between 2008 and 2010, nearly 50,000 ED visits were attributed to rape. Approximately 65% of rape victims resided in geographic areas with low income levels. The majority of patients were aged 18 to 29 (42%) or younger than 18 (29%). The average ED charge attributed to rape was more than $2,000, and the average hospital charge for admitted patients was over $31,000.
Take Home Pearls: Rape appears to be a significant cause of ED visits and remains an important public health issue. Data show that rape is associated with substantial hospital resource utilization.
Injury Due to Legal Intervention
The Particulars: In EDs, it is not uncommon for violence to necessitate legal interventions. However, outcomes or subsequent injuries have been poorly described in published studies.
Data Breakdown: Researchers analyzed national data for all ED visits for injuries due to legal interventions from 2008 to 2010 in a study. More than 170,000 ED visits were due to legal interventions. The table below depicts several characteristics of these visits:
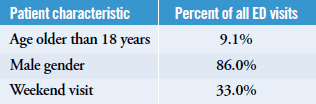
Patients aged 18 to 29 accounted for 40.1% of all ED visits. The average ED charge due to legal interventions was nearly $2,000, and the average hospital charge for those who were admitted was nearly $60,000.
Take Home Pearls: Legal interventions that lead to injuries requiring medical care appear to be a common reason for ED visits. Hospital resource utilization for these visits is high, and certain groups of patients appear to be at greater risk.
EMR Alerts for Severe Sepsis in the ED
The Particulars: Early recognition and treatment of severe sepsis or septic shock has been associated with improved outcomes in previous studies. A setting within an electronic medical record (EMR) that flags healthcare providers with two alerts may help improve processes of care and outcomes among ED patients who develop sepsis or septic shock.
Data Breakdown: Researchers conducted a single-center, before-and-after study of a Severe Sepsis Best Practice Alert (SS-BPA) that was implemented into an EMR. One alert was based on severe sepsis criteria, and a second alert was based on systemic inflammatory response syndrome criteria. During the 7 months following implementation of SS-BPA, timeto- antibiotics was significantly lower, and the proportion of patients who received antibiotics within 60 minutes was higher when compared with the 7 months prior to implementation. The authors note the length of stay (LOS), but not in-hospital mortality, was reduced significantly following SS-BPA implementation.
Take Home Pearl: Implementation of EMR-based best practice alerts for severe sepsis and septic shock among ED patients appears to improve time-to-antibiotic administration and reduce hospital LOS.